ISSN 0439-755X
CN 11-1911/B
主办:中国心理学会
中国科学院心理研究所
出版:科学出版社
CN 11-1911/B
主办:中国心理学会
中国科学院心理研究所
出版:科学出版社
心理学报 ›› 2024, Vol. 56 ›› Issue (10): 1351-1366.doi: 10.3724/SP.J.1041.2024.01351 cstr: 32110.14.2024.01351
杜夏雨, 赖丽足, 史从戎, 郭子涵, 韩菁, 张涛, 任志洪( )
)
收稿日期:2023-07-05
发布日期:2024-07-10
出版日期:2024-10-25
通讯作者:
任志洪, E-mail: ren@ccnu.edu.cn基金资助:
DU Xiayu, LAI Lizu, SHI Congrong, GUO Zihan, HAN Jing, ZHANG Tao, REN Zhihong()
Received:2023-07-05
Online:2024-07-10
Published:2024-10-25
摘要:
本研究旨在考察移动网络化解释偏向矫正(internet-based Cognitive Bias Modification-Interpretation, iCBM-I)对健康焦虑的干预效果、影响因素及灾难化解释在干预起效中的机制作用。采用随机对照试验, 将符合健康焦虑标准的被试(N = 228)随机分配到iCBM-I干预组(100%积极反馈, N = 76)、注意控制组(50%积极50%消极反馈, N = 76)以及等待组(N = 76)。干预组和注意控制组进行为期12天的在线任务训练, 等待组不做训练。在干预前、干预后及干预后一个月对被试的健康焦虑、灾难化解释、一般焦虑和抑郁进行测量。 结果发现: 与等待组相比, iCBM-I干预对健康焦虑个体的灾难化解释、一般焦虑和抑郁症状存在显著的即时效果和一个月后的追踪效果; 基于潜在增长曲线模型的纵向中介检验显示, 相对于注意控制组, iCBM-I干预通过降低个体的灾难化解释进而改善健康焦虑。本研究为健康焦虑的网络化干预提供了新视角, 未来研究可以考虑联合“自上而下”和“自下而上”的干预方法, 以提高健康焦虑的干预效果。
中图分类号:
杜夏雨, 赖丽足, 史从戎, 郭子涵, 韩菁, 张涛, 任志洪. (2024). 健康焦虑的移动网络化解释偏向矫正: 一项随机对照试验. 心理学报, 56(10), 1351-1366.
DU Xiayu, LAI Lizu, SHI Congrong, GUO Zihan, HAN Jing, ZHANG Tao, REN Zhihong. (2024). Internet-based cognitive bias modification of interpretation in health anxiety: A randomized controlled trial. Acta Psychologica Sinica, 56(10), 1351-1366.
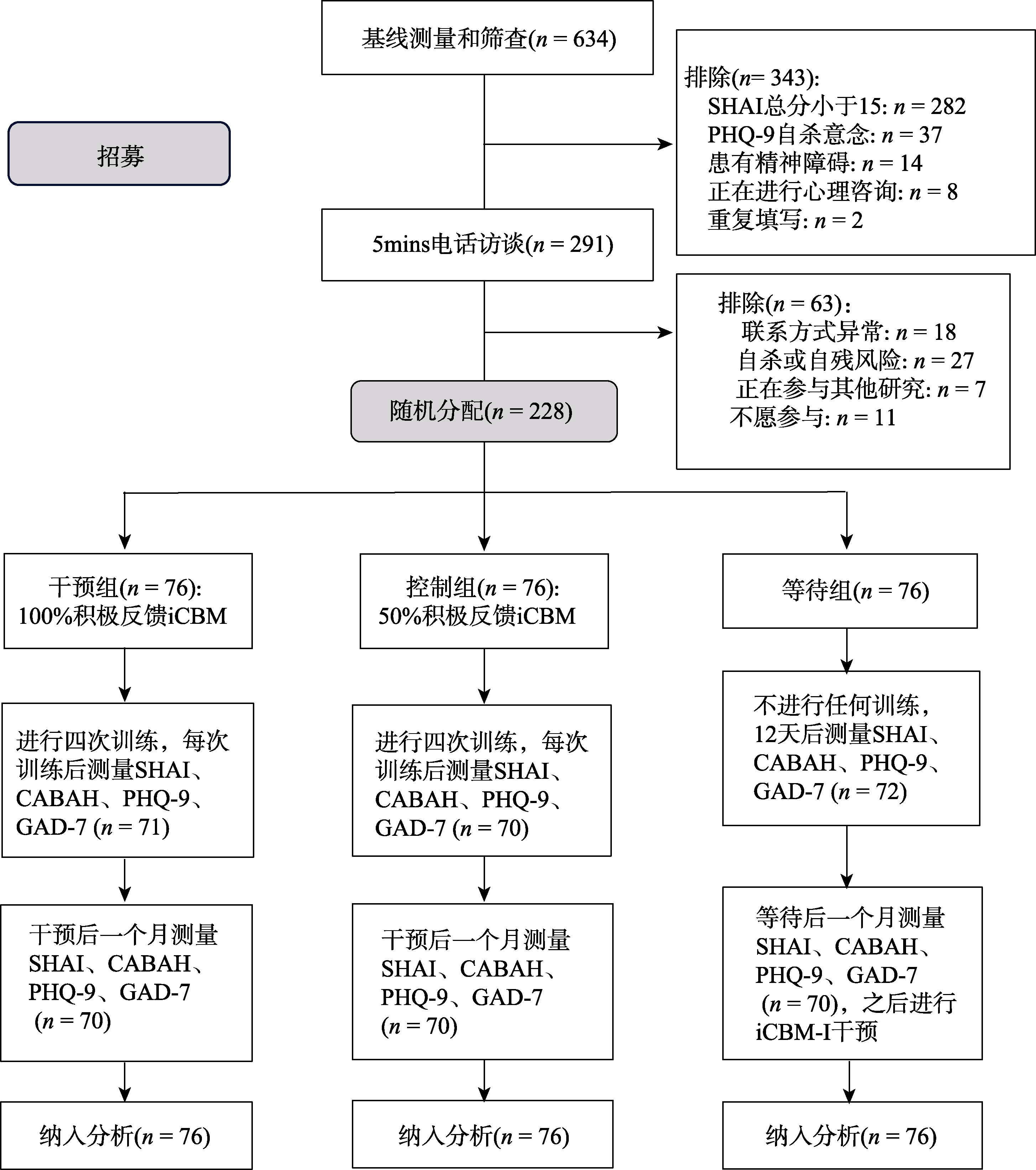
图1 被试筛选及干预流程图 注: SHAI: 简式健康焦虑量表; CABAH: 躯体与健康认知量表; PHQ-9: 患者健康问卷; GAD-7: 广泛性焦虑障碍量表。
| 结果 变量 | 干预组(n = 76) | 控制组(n = 76) | 等待组(n = 76) | 组间差异 | 组间效应量(Cohen's d, 95% CI) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | F (2, 671) | 干预组vs.等待组 | 控制组vs.等待组 | 干预组vs.控制组 | ||
| SHAI | 基线 | 27.64 | 8.53 | 28.20 | 9.95 | 29.45 | 8.75 | 0.852 | −0.21(−0.53, 0.11) | −0.14(−0.46, 0.17) | −0.07(−0.38, 0.25) |
| 后测 | 22.41 | 9.03 | 26.64 | 9.41 | 24.27 | 8.51 | 4.767** | −0.21(−0.53, 0.11) | 0.27(−0.05, 0.59) | −0.50(−0.82, −0.18) | |
| 追踪 | 19.98 | 9.14 | 22.17 | 8.92 | 25.11 | 8.69 | 6.574** | −0.59(−0.91, −0.26) | −0.34(−0.66, −0.02) | −0.26(−0.58, 0.06) | |
| CABAH | 基线 | 36.54 | 6.07 | 36.79 | 6.40 | 35.00 | 6.31 | 2.343 | 0.28(−0.04, 0.60) | 0.33(0.01, 0.65) | −0.05(−0.36, 0.27) |
| 后测 | 29.22 | 6.74 | 32.22 | 6.47 | 33.77 | 5.60 | 13.835*** | −0.83(−1.16, −0.50) | −0.28(−0.60, 0.04) | −0.56(−0.89, −0.24) | |
| 追踪 | 29.87 | 7.30 | 32.48 | 6.20 | 34.05 | 5.97 | 11.471*** | −0.76(−1.09, −0.44) | −0.29(−0.61, 0.03) | −0.49(−0.81, −0.17) | |
| PHQ-9 | 基线 | 19.12 | 4.95 | 19.80 | 5.71 | 20.33 | 4.97 | 1.063 | −0.23(−0.55, 0.08) | −0.10(−0.42, 0.22) | −0.14(−0.45, 0.18) |
| 后测 | 15.79 | 4.12 | 17.29 | 5.46 | 20.59 | 4.74 | 17.244*** | −0.94(−1.27, −0.60) | −0.64(−0.97, −0.32) | −0.30(−0.62, 0.02) | |
| 追踪 | 16.72 | 4.35 | 18.26 | 5.75 | 20.64 | 4.10 | 11.212*** | −0.77(−1.10, −0.44) | −0.46(−0.79, −0.14) | −0.31(−0.63, 0.01) | |
| GAD-7 | 基线 | 15.31 | 4.50 | 15.36 | 4.72 | 15.98 | 4.66 | 0.510 | −0.15(−0.47, 0.17) | −0.14(−0.45, 0.18) | −0.01(−0.33, 0.31) |
| 后测 | 12.46 | 3.95 | 14.09 | 4.60 | 15.26 | 3.92 | 7.536** | −0.62(−0.95, −0.30) | −0.26(−0.58, 0.06) | −0.38(−0.70, −0.06) | |
| 追踪 | 12.71 | 4.36 | 13.55 | 4.42 | 15.23 | 3.75 | 6.103** | −0.56(−0.88, −0.24) | −0.37(−0.69, −0.05) | −0.19(−051, 0.12) | |
表1 基于意向治疗分析的差异检验和干预效果量
| 结果 变量 | 干预组(n = 76) | 控制组(n = 76) | 等待组(n = 76) | 组间差异 | 组间效应量(Cohen's d, 95% CI) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | F (2, 671) | 干预组vs.等待组 | 控制组vs.等待组 | 干预组vs.控制组 | ||
| SHAI | 基线 | 27.64 | 8.53 | 28.20 | 9.95 | 29.45 | 8.75 | 0.852 | −0.21(−0.53, 0.11) | −0.14(−0.46, 0.17) | −0.07(−0.38, 0.25) |
| 后测 | 22.41 | 9.03 | 26.64 | 9.41 | 24.27 | 8.51 | 4.767** | −0.21(−0.53, 0.11) | 0.27(−0.05, 0.59) | −0.50(−0.82, −0.18) | |
| 追踪 | 19.98 | 9.14 | 22.17 | 8.92 | 25.11 | 8.69 | 6.574** | −0.59(−0.91, −0.26) | −0.34(−0.66, −0.02) | −0.26(−0.58, 0.06) | |
| CABAH | 基线 | 36.54 | 6.07 | 36.79 | 6.40 | 35.00 | 6.31 | 2.343 | 0.28(−0.04, 0.60) | 0.33(0.01, 0.65) | −0.05(−0.36, 0.27) |
| 后测 | 29.22 | 6.74 | 32.22 | 6.47 | 33.77 | 5.60 | 13.835*** | −0.83(−1.16, −0.50) | −0.28(−0.60, 0.04) | −0.56(−0.89, −0.24) | |
| 追踪 | 29.87 | 7.30 | 32.48 | 6.20 | 34.05 | 5.97 | 11.471*** | −0.76(−1.09, −0.44) | −0.29(−0.61, 0.03) | −0.49(−0.81, −0.17) | |
| PHQ-9 | 基线 | 19.12 | 4.95 | 19.80 | 5.71 | 20.33 | 4.97 | 1.063 | −0.23(−0.55, 0.08) | −0.10(−0.42, 0.22) | −0.14(−0.45, 0.18) |
| 后测 | 15.79 | 4.12 | 17.29 | 5.46 | 20.59 | 4.74 | 17.244*** | −0.94(−1.27, −0.60) | −0.64(−0.97, −0.32) | −0.30(−0.62, 0.02) | |
| 追踪 | 16.72 | 4.35 | 18.26 | 5.75 | 20.64 | 4.10 | 11.212*** | −0.77(−1.10, −0.44) | −0.46(−0.79, −0.14) | −0.31(−0.63, 0.01) | |
| GAD-7 | 基线 | 15.31 | 4.50 | 15.36 | 4.72 | 15.98 | 4.66 | 0.510 | −0.15(−0.47, 0.17) | −0.14(−0.45, 0.18) | −0.01(−0.33, 0.31) |
| 后测 | 12.46 | 3.95 | 14.09 | 4.60 | 15.26 | 3.92 | 7.536** | −0.62(−0.95, −0.30) | −0.26(−0.58, 0.06) | −0.38(−0.70, −0.06) | |
| 追踪 | 12.71 | 4.36 | 13.55 | 4.42 | 15.23 | 3.75 | 6.103** | −0.56(−0.88, −0.24) | −0.37(−0.69, −0.05) | −0.19(−051, 0.12) | |
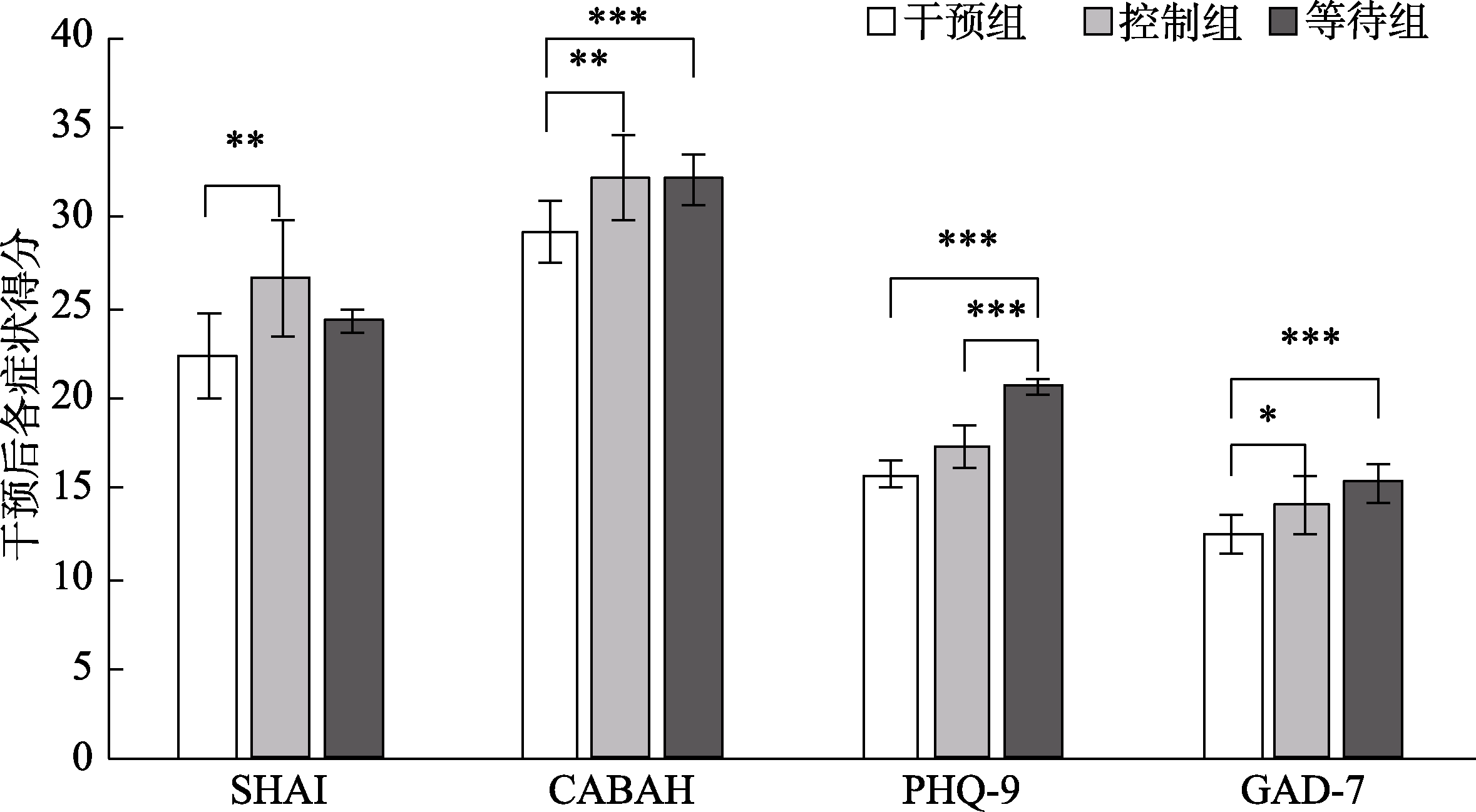
图2 干预后组间差异图 注: SHAI: 简式健康焦虑量表; CABAH: 躯体与健康认知量表; PHQ-9: 患者健康问卷; GAD-7: 广泛性焦虑障碍量表。* p < 0.05, ** p < 0.01, *** p < 0.001
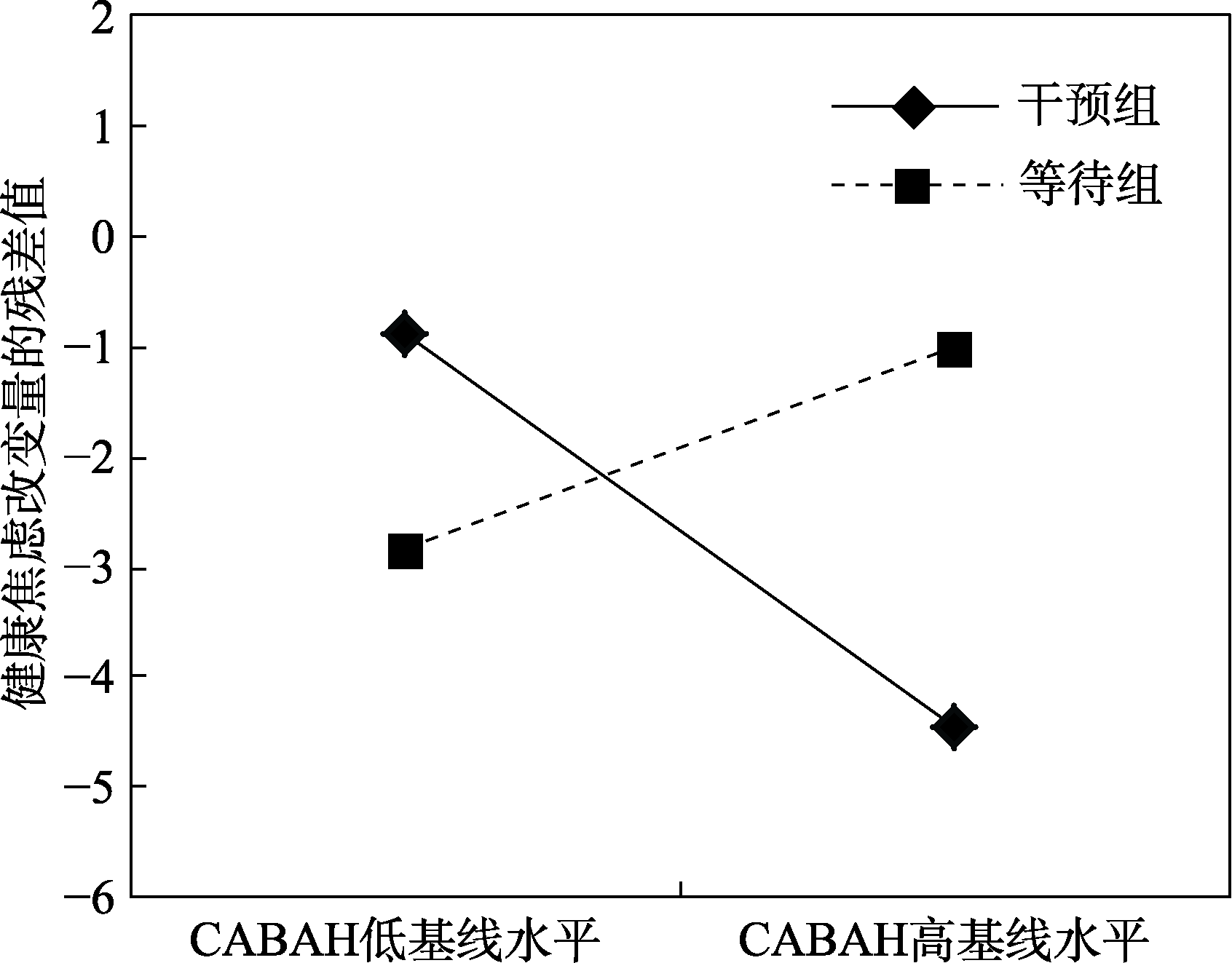
图3 组别与CABAH基线水平对ΔSHAI的交互作用
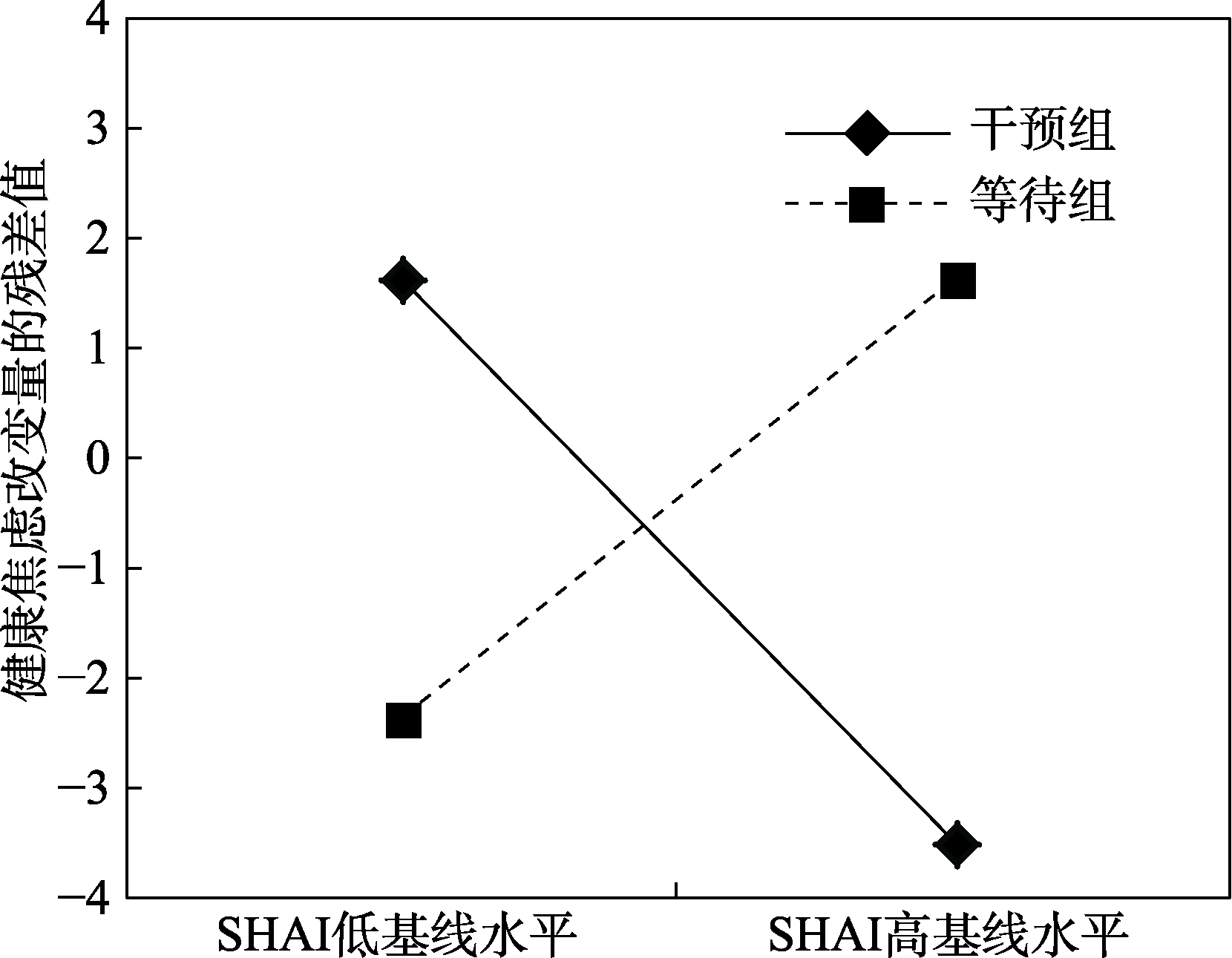
图4 组别与SHAI基线水平对ΔSHAI的交互作用
| 模型 | χ2(df) | χ2/df | SRMR | CFI | AIC | BIC |
|---|---|---|---|---|---|---|
| 参照 | — | < 3 | < 0.08 | > 0.95 | — | — |
| SHAI | ||||||
| 无增长模型 | 98.29(13)*** | 7.56 | 0.25 | 0.82 | 4886.13 | 4907.29 |
| 线性增长模型 | 49.61(10)*** | 4.96 | 0.14 | 0.92 | 4843.45 | 4873.69 |
| 二次增长模型 | 11.26(6) | 1.88 | 0.06 | 0.99 | 4813.09 | 4855.43 |
| 潜在基础增长模型 | 33.31(7)*** | 4.76 | 0.04 | 0.95 | 4833.15 | 4872.46 |
| CABAH | ||||||
| 无增长模型 | 96.27(13)*** | 7.41 | 0.27 | 0.84 | 4308.65 | 4329.82 |
| 线性增长模型 | 28.63(10)** | 2.86 | 0.11 | 0.96 | 4247.01 | 4277.25 |
| 二次增长模型 | 10.24(6) | 1.71 | 0.05 | 0.99 | 4236.61 | 4278.95 |
| 潜在基础增长模型 | 14.70(7)* | 2.10 | 0.03 | 0.99 | 4239.08 | 4278.39 |
表2 SHAI和CABAH变化轨迹检验指标
| 模型 | χ2(df) | χ2/df | SRMR | CFI | AIC | BIC |
|---|---|---|---|---|---|---|
| 参照 | — | < 3 | < 0.08 | > 0.95 | — | — |
| SHAI | ||||||
| 无增长模型 | 98.29(13)*** | 7.56 | 0.25 | 0.82 | 4886.13 | 4907.29 |
| 线性增长模型 | 49.61(10)*** | 4.96 | 0.14 | 0.92 | 4843.45 | 4873.69 |
| 二次增长模型 | 11.26(6) | 1.88 | 0.06 | 0.99 | 4813.09 | 4855.43 |
| 潜在基础增长模型 | 33.31(7)*** | 4.76 | 0.04 | 0.95 | 4833.15 | 4872.46 |
| CABAH | ||||||
| 无增长模型 | 96.27(13)*** | 7.41 | 0.27 | 0.84 | 4308.65 | 4329.82 |
| 线性增长模型 | 28.63(10)** | 2.86 | 0.11 | 0.96 | 4247.01 | 4277.25 |
| 二次增长模型 | 10.24(6) | 1.71 | 0.05 | 0.99 | 4236.61 | 4278.95 |
| 潜在基础增长模型 | 14.70(7)* | 2.10 | 0.03 | 0.99 | 4239.08 | 4278.39 |
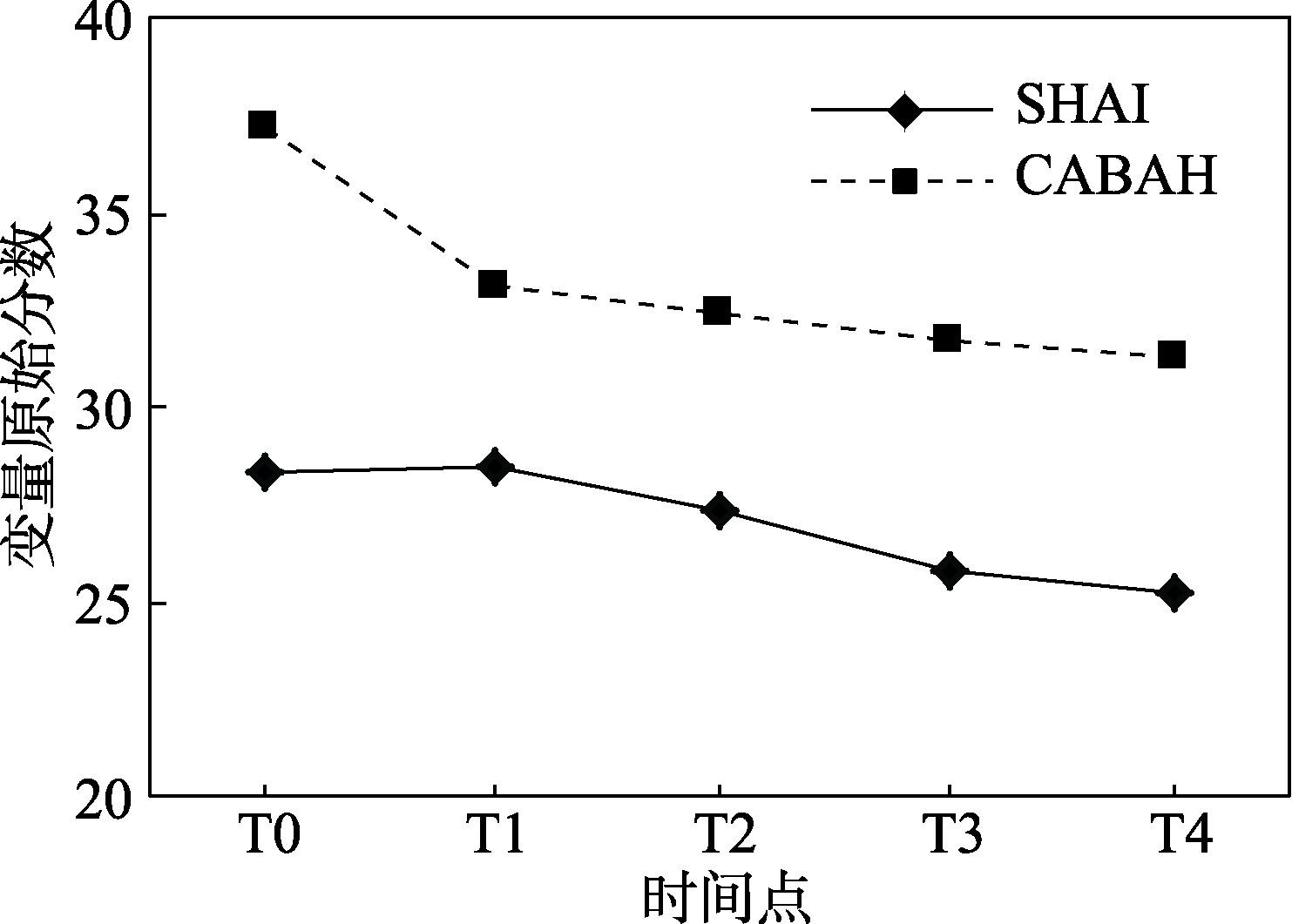
图5 健康焦虑和灾难化解释随时间的变化轨迹
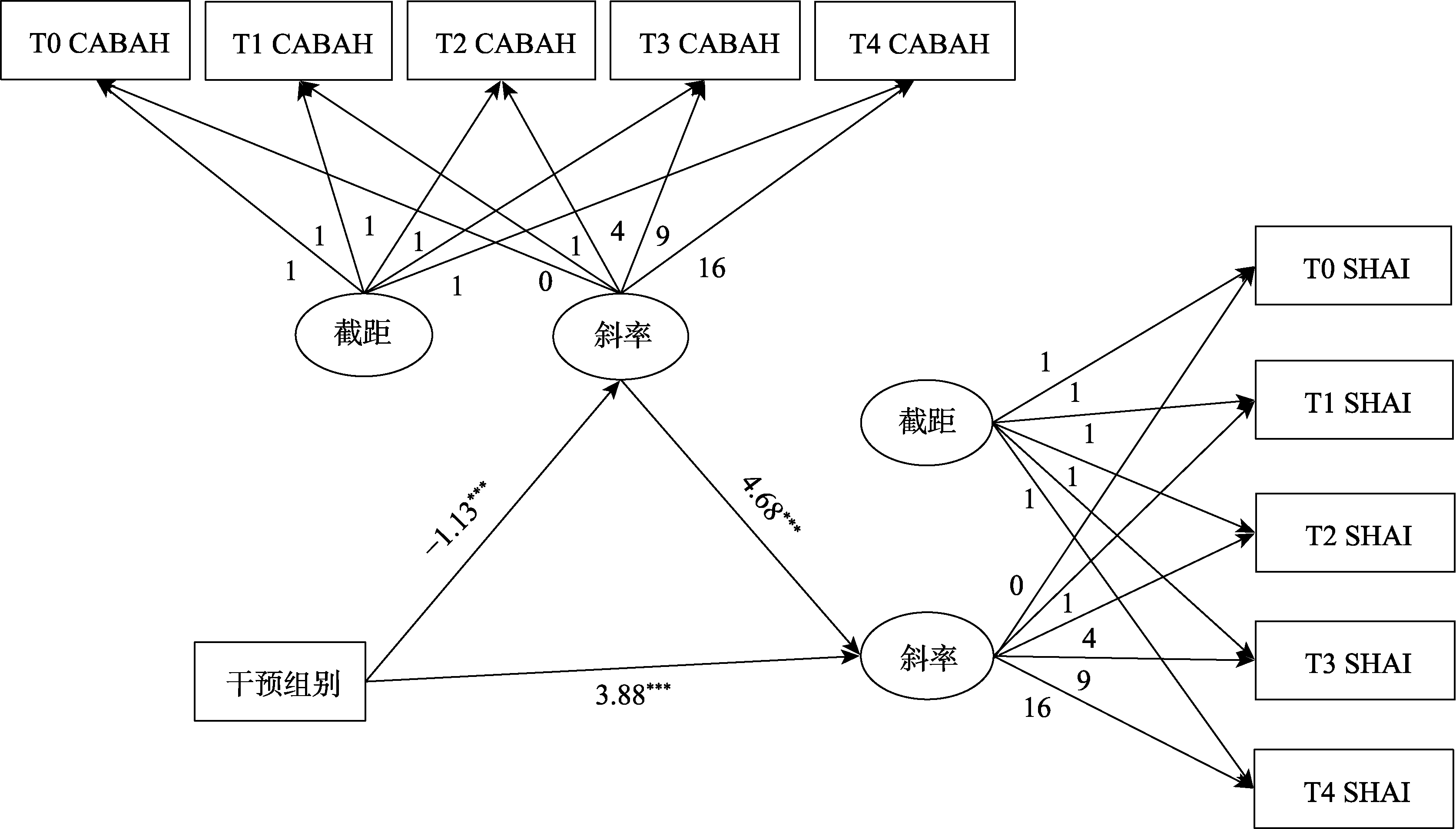
图6 灾难化解释的纵向中介模型 注: *** p < 0.001
| 段落/标题 | 条目号 | 核查单条目描述 | 页码 | |
|---|---|---|---|---|
| 标题和摘要 | ||||
| 1a | 文题中能确认是随机化的试验 | p1351 | ||
| 1b | 用结构式摘要概括试验设计、方法、结果和结论 | p1351 | ||
| 引言 | ||||
| 背景和目的 | 2a | 研究课题的科学背景和原理的解释 | p1351−1353 | |
| 2b | 研究课题的特定目的或假设 | p1353 | ||
| 方法 | ||||
| 试验设计 | 3a | 描述包括分配比例的试验设计(例如平行设计、析因设计) | p1354 | |
| 3b | 试验启动后方法上的重要改变及理由(例如合格标准) | NA | ||
| 受试者 | 4a | 参加者的合格标准 | p1354 | |
| 4b | 资料收集的环境和地点 | p1354 | ||
| 干预方法 | 5 | 各组干预措施的详细情况以及实际实施的方法和时间, 以便重复试验 | p1354−1356 | |
| 结局指标 | 6a | 明确定义事先确定的主要和次要结局指标, 包括测评的方法和时间 | p1354 | |
| 6b | 试验启动后试验结局的任何改变及理由 | NA | ||
| 样本量 | 7a | 样本量是如何确定的 | p1354 | |
| 7b | 进行任何的中期分析都应给予解释, 并给出终止试验的原则 | NA | ||
| 随机序列生成 | 8a | 用于产生随机分配顺序的方法 | p1355 | |
| 8b | 随机化类型, 任何限定细节(例如区组化和各区组样本大小) | p1355 | ||
| 分配隐藏 | 9 | 用于实施随机分配顺序的方法(例如按顺序编号的容器), 说明分配干预之前所采取隐藏顺序的步骤 | p1355 | |
| 实施 | 10 | 谁产生的分配顺序, 谁入选的受试者, 谁将受试者分到各干预组 | p1355 | |
| 盲法 | 11a | 如果使用了盲法, 分配干预后谁处于盲态(例如受试者、保健提供者和结局评估者) | p1355 | |
| 11b | 描述干预的相似性情况 | p1355 | ||
| 统计学方法 | 12a | 用于比较各组主要和次要结局的统计学方法 | p1356 | |
| 12b | 额外分析方法, 例如亚组分析和校正分析 | p1356−1357 | ||
| 结果 | ||||
| 受试者纳入流程 | 13a | 每组被随机分配、接受预期处理及分析主要结局的人数 | p1357 | |
| 13b | 每组随机化后丢失和剔除的情况及理由 | NA | ||
| 招募情况 | 14a | 用日期来明确招募和随访的时间 | p1355 | |
| 14b | 为什么试验结束了或者暂停了下来 | NA | ||
| 基线数据 | 15 | 用表格显示各组的基线人口统计学资料和临床特征 | p1358 | |
| 纳入分析的受试者数量 | 16 | 分析每次纳入到各组的受试者例数(分母), 而不管是否用了原来的分组 | p1357−1358 | |
| 结局和效应估计 | 17a | 各组每一个主要和次要结局结果、估计的效应大小及其精度(例如95%置信区间) | p1357−1358 | |
| 17b | 对两分类的结局, 推荐绝对的和相对的效应大小两者兼用 | p1357−1358 | ||
| 辅助分析 | 18 | 报告所进行的任何其他分析, 包括亚组分析、校正分析, 并区分开哪些是预定的?哪些是探索性的? | p1358−1360 | |
| 不良反应 | 19 | 每组所有的重要危害或非预期的效应 | NA | |
| 讨论 | ||||
| 局限性 | 20 | 试验的局限性, 说明潜在偏倚、不够准确的来源, 可能还有分析的多样性 | p1362 | |
| 可推广性 | 21 | 试验结果的可推广性(外部有效性、适用性) | p1368 | |
| 解释 | 22 | 给出与结果一致的解释, 在受益和伤害间进行平衡, 考虑其他的相关证据 | p1360−1362 | |
| 其他信息 | ||||
| 注册 | 23 | 试验注册的注册号和名称 | p1354 | |
| 研究方案 | 24 | 需要时在哪里可以获取完整的试验方案 | p1354−1356 | |
| 基金资助 | 25 | 资助的来源和其他的支持(例如药品供应), 资助者的作用 | p1351 | |
附表1 2010年版CONSORT声明——报告平行组随机试验的项目核查单
| 段落/标题 | 条目号 | 核查单条目描述 | 页码 | |
|---|---|---|---|---|
| 标题和摘要 | ||||
| 1a | 文题中能确认是随机化的试验 | p1351 | ||
| 1b | 用结构式摘要概括试验设计、方法、结果和结论 | p1351 | ||
| 引言 | ||||
| 背景和目的 | 2a | 研究课题的科学背景和原理的解释 | p1351−1353 | |
| 2b | 研究课题的特定目的或假设 | p1353 | ||
| 方法 | ||||
| 试验设计 | 3a | 描述包括分配比例的试验设计(例如平行设计、析因设计) | p1354 | |
| 3b | 试验启动后方法上的重要改变及理由(例如合格标准) | NA | ||
| 受试者 | 4a | 参加者的合格标准 | p1354 | |
| 4b | 资料收集的环境和地点 | p1354 | ||
| 干预方法 | 5 | 各组干预措施的详细情况以及实际实施的方法和时间, 以便重复试验 | p1354−1356 | |
| 结局指标 | 6a | 明确定义事先确定的主要和次要结局指标, 包括测评的方法和时间 | p1354 | |
| 6b | 试验启动后试验结局的任何改变及理由 | NA | ||
| 样本量 | 7a | 样本量是如何确定的 | p1354 | |
| 7b | 进行任何的中期分析都应给予解释, 并给出终止试验的原则 | NA | ||
| 随机序列生成 | 8a | 用于产生随机分配顺序的方法 | p1355 | |
| 8b | 随机化类型, 任何限定细节(例如区组化和各区组样本大小) | p1355 | ||
| 分配隐藏 | 9 | 用于实施随机分配顺序的方法(例如按顺序编号的容器), 说明分配干预之前所采取隐藏顺序的步骤 | p1355 | |
| 实施 | 10 | 谁产生的分配顺序, 谁入选的受试者, 谁将受试者分到各干预组 | p1355 | |
| 盲法 | 11a | 如果使用了盲法, 分配干预后谁处于盲态(例如受试者、保健提供者和结局评估者) | p1355 | |
| 11b | 描述干预的相似性情况 | p1355 | ||
| 统计学方法 | 12a | 用于比较各组主要和次要结局的统计学方法 | p1356 | |
| 12b | 额外分析方法, 例如亚组分析和校正分析 | p1356−1357 | ||
| 结果 | ||||
| 受试者纳入流程 | 13a | 每组被随机分配、接受预期处理及分析主要结局的人数 | p1357 | |
| 13b | 每组随机化后丢失和剔除的情况及理由 | NA | ||
| 招募情况 | 14a | 用日期来明确招募和随访的时间 | p1355 | |
| 14b | 为什么试验结束了或者暂停了下来 | NA | ||
| 基线数据 | 15 | 用表格显示各组的基线人口统计学资料和临床特征 | p1358 | |
| 纳入分析的受试者数量 | 16 | 分析每次纳入到各组的受试者例数(分母), 而不管是否用了原来的分组 | p1357−1358 | |
| 结局和效应估计 | 17a | 各组每一个主要和次要结局结果、估计的效应大小及其精度(例如95%置信区间) | p1357−1358 | |
| 17b | 对两分类的结局, 推荐绝对的和相对的效应大小两者兼用 | p1357−1358 | ||
| 辅助分析 | 18 | 报告所进行的任何其他分析, 包括亚组分析、校正分析, 并区分开哪些是预定的?哪些是探索性的? | p1358−1360 | |
| 不良反应 | 19 | 每组所有的重要危害或非预期的效应 | NA | |
| 讨论 | ||||
| 局限性 | 20 | 试验的局限性, 说明潜在偏倚、不够准确的来源, 可能还有分析的多样性 | p1362 | |
| 可推广性 | 21 | 试验结果的可推广性(外部有效性、适用性) | p1368 | |
| 解释 | 22 | 给出与结果一致的解释, 在受益和伤害间进行平衡, 考虑其他的相关证据 | p1360−1362 | |
| 其他信息 | ||||
| 注册 | 23 | 试验注册的注册号和名称 | p1354 | |
| 研究方案 | 24 | 需要时在哪里可以获取完整的试验方案 | p1354−1356 | |
| 基金资助 | 25 | 资助的来源和其他的支持(例如药品供应), 资助者的作用 | p1351 | |
| 变量 | 干预组(n = 76) | 控制组(n = 76) | 等待组(n = 76) | 总计(n = 228) | F/χ2 | p | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M/N | SD/% | M/N | SD/% | M/N | SD/% | M/N | SD/% | |||||||
| 年龄 | 22.38 | 4.026 | 22.42 | 3.685 | 23.37 | 4.230 | 22.72 | 3.995 | 1.493 | 0.227 | ||||
| 性别 | 1.826 | 0.401 | ||||||||||||
| 男 | 28 | 36.8% | 33 | 43.4% | 25 | 32.9% | 86 | 37.7% | v | |||||
| 女 | 48 | 63.2% | 43 | 56.6% | 51 | 67.1% | 142 | 62.3% | ||||||
| 常住地 | 0.058 | 1.000 | ||||||||||||
| 农村 | 14 | 18.4% | 15 | 19.7% | 14 | 18.4% | 43 | 18.9% | ||||||
| 城市 | 57 | 75.0% | 56 | 73.7% | 57 | 75.0% | 170 | 74.6% | ||||||
| 郊区 | 5 | 6.6% | 5 | 6.6% | 5 | 6.6% | 15 | 6.6% | ||||||
| 受教育程度 | 15.085 | 0.020 | ||||||||||||
| 高中及以下 | 3 | 3.9% | 2 | 2.6% | 1 | 1.3% | 6 | 2.6% | ||||||
| 大专 | 8 | 10.5% | 7 | 9.2% | 3 | 3.9% | 18 | 7.9% | ||||||
| 本科 | 56 | 73.7% | 58 | 76.3% | 48 | 63.2% | 162 | 71.1% | ||||||
| 硕士及以上 | 9 | 11.8% | 9 | 11.8% | 24 | 31.6% | 42 | 18.4% | ||||||
| 婚姻状况 | 0.427 | 0.980 | ||||||||||||
| 已婚/同居 | 5 | 6.6% | 4 | 5.3% | 5 | 6.6% | 14 | 6.1% | ||||||
| 恋爱中 | 24 | 31.6% | 26 | 34.2% | 27 | 35.5% | 77 | 33.8% | ||||||
| 单身 | 47 | 61.8% | 46 | 60.5% | 44 | 57.9% | 137 | 60.1% | ||||||
| 工作状况 | 8.339 | 0.214 | ||||||||||||
| 全职工作 | 18 | 23.7% | 18 | 23.7% | 20 | 26.3% | 56 | 24.6% | ||||||
| 兼职工作 | 5 | 6.6% | 4 | 5.3% | 1 | 1.3% | 10 | 4.4% | ||||||
| 无稳定工作 | 2 | 2.6% | 0 | 0 | 5 | 6.6% | 5 | 3.1% | ||||||
| 在校学生 | 51 | 67.1% | 54 | 71.1% | 50 | 65.8% | 155 | 68.0% | ||||||
| 收入状况 | 5.437 | 0.489 | ||||||||||||
| 完全满足 | 10 | 13.2% | 14 | 18.4% | 13 | 17.1% | 37 | 16.2% | ||||||
| 基本满足 | 52 | 68.4% | 51 | 67.1% | 53 | 69.7% | 156 | 68.4% | ||||||
| 基本不满足 | 10 | 13.2% | 9 | 11.8% | 4 | 5.3% | 23 | 10.1% | ||||||
| 完全不满足 | 4 | 5.3% | 2 | 2.6% | 6 | 7.9% | 12 | 5.3% | ||||||
| 基线症状 | ||||||||||||||
| SHAI | 27.93 | 8.53 | 28.79 | 9.95 | 28.25 | 8.75 | 28.32 | 9.07 | 0.172 | 0.842 | ||||
| CABAH | 36.91 | 6.07 | 37.49 | 6.40 | 33.36 | 6.31 | 35.92 | 6.50 | 9.702 | < 0.001 | ||||
| PHQ-9 | 18.96 | 4.95 | 19.67 | 5.71 | 19.61 | 4.97 | 19.41 | 5.21 | 0.429 | 0.651 | ||||
| GAD-7 | 15.62 | 4.50 | 15.75 | 4.72 | 16.14 | 4.66 | 15.84 | 4.61 | 0.266 | 0.766 | ||||
附表2 样本基本特征
| 变量 | 干预组(n = 76) | 控制组(n = 76) | 等待组(n = 76) | 总计(n = 228) | F/χ2 | p | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M/N | SD/% | M/N | SD/% | M/N | SD/% | M/N | SD/% | |||||||
| 年龄 | 22.38 | 4.026 | 22.42 | 3.685 | 23.37 | 4.230 | 22.72 | 3.995 | 1.493 | 0.227 | ||||
| 性别 | 1.826 | 0.401 | ||||||||||||
| 男 | 28 | 36.8% | 33 | 43.4% | 25 | 32.9% | 86 | 37.7% | v | |||||
| 女 | 48 | 63.2% | 43 | 56.6% | 51 | 67.1% | 142 | 62.3% | ||||||
| 常住地 | 0.058 | 1.000 | ||||||||||||
| 农村 | 14 | 18.4% | 15 | 19.7% | 14 | 18.4% | 43 | 18.9% | ||||||
| 城市 | 57 | 75.0% | 56 | 73.7% | 57 | 75.0% | 170 | 74.6% | ||||||
| 郊区 | 5 | 6.6% | 5 | 6.6% | 5 | 6.6% | 15 | 6.6% | ||||||
| 受教育程度 | 15.085 | 0.020 | ||||||||||||
| 高中及以下 | 3 | 3.9% | 2 | 2.6% | 1 | 1.3% | 6 | 2.6% | ||||||
| 大专 | 8 | 10.5% | 7 | 9.2% | 3 | 3.9% | 18 | 7.9% | ||||||
| 本科 | 56 | 73.7% | 58 | 76.3% | 48 | 63.2% | 162 | 71.1% | ||||||
| 硕士及以上 | 9 | 11.8% | 9 | 11.8% | 24 | 31.6% | 42 | 18.4% | ||||||
| 婚姻状况 | 0.427 | 0.980 | ||||||||||||
| 已婚/同居 | 5 | 6.6% | 4 | 5.3% | 5 | 6.6% | 14 | 6.1% | ||||||
| 恋爱中 | 24 | 31.6% | 26 | 34.2% | 27 | 35.5% | 77 | 33.8% | ||||||
| 单身 | 47 | 61.8% | 46 | 60.5% | 44 | 57.9% | 137 | 60.1% | ||||||
| 工作状况 | 8.339 | 0.214 | ||||||||||||
| 全职工作 | 18 | 23.7% | 18 | 23.7% | 20 | 26.3% | 56 | 24.6% | ||||||
| 兼职工作 | 5 | 6.6% | 4 | 5.3% | 1 | 1.3% | 10 | 4.4% | ||||||
| 无稳定工作 | 2 | 2.6% | 0 | 0 | 5 | 6.6% | 5 | 3.1% | ||||||
| 在校学生 | 51 | 67.1% | 54 | 71.1% | 50 | 65.8% | 155 | 68.0% | ||||||
| 收入状况 | 5.437 | 0.489 | ||||||||||||
| 完全满足 | 10 | 13.2% | 14 | 18.4% | 13 | 17.1% | 37 | 16.2% | ||||||
| 基本满足 | 52 | 68.4% | 51 | 67.1% | 53 | 69.7% | 156 | 68.4% | ||||||
| 基本不满足 | 10 | 13.2% | 9 | 11.8% | 4 | 5.3% | 23 | 10.1% | ||||||
| 完全不满足 | 4 | 5.3% | 2 | 2.6% | 6 | 7.9% | 12 | 5.3% | ||||||
| 基线症状 | ||||||||||||||
| SHAI | 27.93 | 8.53 | 28.79 | 9.95 | 28.25 | 8.75 | 28.32 | 9.07 | 0.172 | 0.842 | ||||
| CABAH | 36.91 | 6.07 | 37.49 | 6.40 | 33.36 | 6.31 | 35.92 | 6.50 | 9.702 | < 0.001 | ||||
| PHQ-9 | 18.96 | 4.95 | 19.67 | 5.71 | 19.61 | 4.97 | 19.41 | 5.21 | 0.429 | 0.651 | ||||
| GAD-7 | 15.62 | 4.50 | 15.75 | 4.72 | 16.14 | 4.66 | 15.84 | 4.61 | 0.266 | 0.766 | ||||
| 变量 | F | df | p |
|---|---|---|---|
| 性别 | 2.158 | (1, 220) | 0.143 |
| 组别 | 5.313 | (2, 220) | 0.006 |
| 性别*组别 | 1.247 | (2, 220) | 0.290 |
| 常住地 | 1.057 | (2, 217) | 0.349 |
| 组别 | 4.585 | (2, 217) | 0.011 |
| 常住地*组别 | 0.345 | (2, 217) | 0.847 |
| 受教育程度 | 1.244 | (2, 218) | 0.290 |
| 组别 | 2.526 | (2, 218) | 0.082 |
| 受教育程度*组别 | 0.414 | (2, 218) | 0.798 |
| 婚姻状况 | 0.213 | (2, 217) | 0.808 |
| 组别 | 6.529 | (2, 217) | 0.002 |
| 婚姻状况*组别 | 1.959 | (2, 217) | 0.102 |
| 工作状况 | 0.133 | (2, 217) | 0.876 |
| 组别 | 1.890 | (2, 217) | 0.154 |
| 工作状况*组别 | 1.965 | (4, 217) | 0.101 |
| 收入状况 | 0.691 | (2, 217) | 0.502 |
| 组别 | 4.304 | (2, 217) | 0.015 |
| 收入状况*组别 | 1.429 | (4, 217) | 0.225 |
附表3.1 人口学分类变量与组别的方差分析
| 变量 | F | df | p |
|---|---|---|---|
| 性别 | 2.158 | (1, 220) | 0.143 |
| 组别 | 5.313 | (2, 220) | 0.006 |
| 性别*组别 | 1.247 | (2, 220) | 0.290 |
| 常住地 | 1.057 | (2, 217) | 0.349 |
| 组别 | 4.585 | (2, 217) | 0.011 |
| 常住地*组别 | 0.345 | (2, 217) | 0.847 |
| 受教育程度 | 1.244 | (2, 218) | 0.290 |
| 组别 | 2.526 | (2, 218) | 0.082 |
| 受教育程度*组别 | 0.414 | (2, 218) | 0.798 |
| 婚姻状况 | 0.213 | (2, 217) | 0.808 |
| 组别 | 6.529 | (2, 217) | 0.002 |
| 婚姻状况*组别 | 1.959 | (2, 217) | 0.102 |
| 工作状况 | 0.133 | (2, 217) | 0.876 |
| 组别 | 1.890 | (2, 217) | 0.154 |
| 工作状况*组别 | 1.965 | (4, 217) | 0.101 |
| 收入状况 | 0.691 | (2, 217) | 0.502 |
| 组别 | 4.304 | (2, 217) | 0.015 |
| 收入状况*组别 | 1.429 | (4, 217) | 0.225 |
| 变量 | β | t | ΔR2 | F | |
|---|---|---|---|---|---|
| 第一步 | 0.007 | 0.808 | |||
| 受教育程度 | 0.047 | -0.168 | |||
| CABAH基线水平 | 0.073 | 1.098 | |||
| 第二步 | 0.051 | 2.719* | |||
| D1 | 0.229 | 3.041** | |||
| D2 | 0.011 | 0.139 | |||
| 年龄 | -0.038 | -0.574 | |||
| 第三步 | 0.003 | 2.029 | |||
| D1×年龄 | -0.072 | -0.789 | |||
| D2×年龄 | -0.059 | -0.619 | |||
| 第一步 | 0.002 | 0.410 | |||
| 受教育程度 | 0.043 | 0.640 | |||
| 第二步 | 0.054 | 3.326* | |||
| D1 | 0.229 | 3.047 | |||
| D2 | 0.007 | 0.093 | |||
| CABAH基线水平 | 0.037 | 0.544 | |||
| 第三步 | 0.021 | 3.091** | |||
| D1×CABAH基线水平 | 0.017 | 0.178 | |||
| D2×CABAH基线水平 | 0.197 | 2.006* | |||
| 第一步 | 0.007 | 0.808 | |||
| 受教育程度 | 0.047 | 0.703 | |||
| CABAH基线水平 | 0.073 | 1.098 | |||
| 第二步 | 0.051 | 2.709* | |||
| D1 | 0.230 | 3.052** | |||
| D2 | 0.014 | 0.177 | |||
| SHAI基线水平 | -0.042 | -0.533 | |||
| 第三步 | 0.054 | 3.955*** | |||
| D1×SHAI基线水平 | 0.070 | 0.715 | |||
| D2×SHAI基线水平 | 0.311 | 3.405** | |||
| 第一步 | 0.007 | 0.808 | |||
| 受教育程度 | 0.047 | 0.703 | |||
| CABAH基线水平 | 0.073 | 1.098 | |||
| 第二步 | 0.085 | 4.492** | |||
| D1 | 0.230 | 3.105** | |||
| D2 | -0.014 | -0.175 | |||
| GAD-7基线水平 | 0.198 | 2.949 | |||
| 第三步 | 0.054 | 3.955*** | |||
| D1×GAD-7基线水平 | 0.061 | 0.658 | |||
| D2×GAD-7基线水平 | 0.126 | 1.351 | |||
| 第一步 | 0.007 | 0.808 | |||
| 受教育程度 | 0.047 | 0.703 | |||
| CABAH基线水平 | 0.073 | 1.098 | |||
| 第二步 | 0.075 | 3.984*** | |||
| D1 | 0.220 | 2.957 | |||
| D2 | -0.019 | -0.237 | |||
| PHQ-9基线水平 | 0.169 | 2.510* | |||
| 第三步 | 0.011 | 3.209*** | |||
| D1×PHQ-9基线水平 | 0.050 | 0.505 | |||
| D2×PHQ-9基线水平 | 0.140 | 1.536 |
附表3.2 年龄、症状基线水平与组别的分层回归分析
| 变量 | β | t | ΔR2 | F | |
|---|---|---|---|---|---|
| 第一步 | 0.007 | 0.808 | |||
| 受教育程度 | 0.047 | -0.168 | |||
| CABAH基线水平 | 0.073 | 1.098 | |||
| 第二步 | 0.051 | 2.719* | |||
| D1 | 0.229 | 3.041** | |||
| D2 | 0.011 | 0.139 | |||
| 年龄 | -0.038 | -0.574 | |||
| 第三步 | 0.003 | 2.029 | |||
| D1×年龄 | -0.072 | -0.789 | |||
| D2×年龄 | -0.059 | -0.619 | |||
| 第一步 | 0.002 | 0.410 | |||
| 受教育程度 | 0.043 | 0.640 | |||
| 第二步 | 0.054 | 3.326* | |||
| D1 | 0.229 | 3.047 | |||
| D2 | 0.007 | 0.093 | |||
| CABAH基线水平 | 0.037 | 0.544 | |||
| 第三步 | 0.021 | 3.091** | |||
| D1×CABAH基线水平 | 0.017 | 0.178 | |||
| D2×CABAH基线水平 | 0.197 | 2.006* | |||
| 第一步 | 0.007 | 0.808 | |||
| 受教育程度 | 0.047 | 0.703 | |||
| CABAH基线水平 | 0.073 | 1.098 | |||
| 第二步 | 0.051 | 2.709* | |||
| D1 | 0.230 | 3.052** | |||
| D2 | 0.014 | 0.177 | |||
| SHAI基线水平 | -0.042 | -0.533 | |||
| 第三步 | 0.054 | 3.955*** | |||
| D1×SHAI基线水平 | 0.070 | 0.715 | |||
| D2×SHAI基线水平 | 0.311 | 3.405** | |||
| 第一步 | 0.007 | 0.808 | |||
| 受教育程度 | 0.047 | 0.703 | |||
| CABAH基线水平 | 0.073 | 1.098 | |||
| 第二步 | 0.085 | 4.492** | |||
| D1 | 0.230 | 3.105** | |||
| D2 | -0.014 | -0.175 | |||
| GAD-7基线水平 | 0.198 | 2.949 | |||
| 第三步 | 0.054 | 3.955*** | |||
| D1×GAD-7基线水平 | 0.061 | 0.658 | |||
| D2×GAD-7基线水平 | 0.126 | 1.351 | |||
| 第一步 | 0.007 | 0.808 | |||
| 受教育程度 | 0.047 | 0.703 | |||
| CABAH基线水平 | 0.073 | 1.098 | |||
| 第二步 | 0.075 | 3.984*** | |||
| D1 | 0.220 | 2.957 | |||
| D2 | -0.019 | -0.237 | |||
| PHQ-9基线水平 | 0.169 | 2.510* | |||
| 第三步 | 0.011 | 3.209*** | |||
| D1×PHQ-9基线水平 | 0.050 | 0.505 | |||
| D2×PHQ-9基线水平 | 0.140 | 1.536 |
| [1] |
Agarwal G., Varghese S., Francis M., & Willan J. (2023). High prevalence of persistent COVID-19-related health anxiety and social restriction in patients with haematological disorders. British Journal of Haematology, 202(5), 1065-1070.
doi: 10.1111/bjh.18960 pmid: 37408108 |
| [2] | Akbari M., Spada M. M., Nikčević A. V., & Zamani E. (2021). The relationship between fear of covid-19 and health anxiety among families with covid-19 infected: The mediating role of metacognitions, intolerance of uncertainty and emotion regulation. Clinical Psychology & Psychotherapy, 28(6), 1354-1366. |
| [3] | Antognelli S. L., Sharrock M. J., & Newby J. M. (2020). A randomised controlled trial of computerised interpretation bias modification for health anxiety. Journal of Behavior Therapy and Experimental Psychiatry, 66, 101518. |
| [4] | Aue T., & Okon-Singer H. (2020). Cognitive biases in health and psychiatric disorders: Neurophysiological foundations. Academic Press. |
| [5] |
Axelsson E., Andersson E., Ljótsson B., Björkander D., Hedman-Lagerlöf M., & Hedman-Lagerlöf E. (2020). Effect of internet vs face-to-face cognitive behavior therapy for health anxiety: A randomized noninferiority clinical trial. JAMA Psychiatry, 77(9), 915-924.
doi: 10.1001/jamapsychiatry.2020.0940 pmid: 32401286 |
| [6] |
Bailey R., & Wells A. (2015). Metacognitive beliefs moderate the relationship between catastrophic misinterpretation and health anxiety. Journal of Anxiety Disorders, 34, 8-14.
doi: 10.1016/j.janxdis.2015.05.005 pmid: 26093824 |
| [7] | Bredemeier K., Church L., Bounoua N., Feler B., & Spielberg J. M. (2023). Intolerance of uncertainty, anxiety sensitivity, and health anxiety during the COVID-19 pandemic: Exploring temporal relationships using cross-lag analysis. Journal of Anxiety Disorders, 93, 102660. |
| [8] |
Brown T. A. (2007). Temporal course and structural relationships among dimensions of temperament and DSM-IV anxiety and mood disorder constructs. Journal of Abnormal Psychology, 116(2), 313-328.
pmid: 17516764 |
| [9] |
Bults M., Beaujean D. J., de Zwart O., Kok G., van Empelen P., van Steenbergen J. E., ... Voeten H. A. (2011). Perceived risk, anxiety, and behavioural responses of the general public during the early phase of the Influenza A (H1N1) pandemic in the Netherlands: Results of three consecutive online surveys. BMC Public Health, 11, 2.
doi: 10.1186/1471-2458-11-2 pmid: 21199571 |
| [10] | Burnham K. P., & Anderson D. R. (2004). Multimodel inference: Understanding AIC and BIC in model selection. Sociological Methods & Research, 33(2), 261-304. |
| [11] | Capron D. W., Norr A. M., Allan N. P., & Schmidt N. B. (2017). Combined “top-down” and “bottom-up” intervention for anxiety sensitivity: Pilot randomized trial testing the additive effect of interpretation bias modification. Journal of Psychiatric Research, 85, 75-82. |
| [12] | Chan F. H. F., Takano K., Lau J. Y. F., & Barry T. J. (2020). Evaluation of the factor structure and content specificity of the interpretation bias task (IBT). Cognitive Therapy and Research, 44(6), 1213-1224. |
| [13] |
Clark D., Beck A., & Brown G. (1989). Cognitive mediation in general psychiatric outpatients: A test of the content- specificity hypothesis. Journal of Personality and Social Psychology, 56(6), 958-964.
pmid: 2746459 |
| [14] |
Dezutter J., Luyckx K., Schaap-Jonker H., Büssing A., Corveleyn J., & Hutsebaut D. (2010). God image and happiness in chronic pain patients: The mediating role of disease interpretation. Pain medicine, 11(5), 765-773.
doi: 10.1111/j.1526-4637.2010.00827.x pmid: 20353410 |
| [15] | Dreier M., Ludwig J., Hrter M., Knesebeck O. V. D., Baumgardt J., Bock T., ... Liebherz S. (2019). Development and evaluation of e-mental health interventions to reduce stigmatization of suicidality: A study protocol. BMC Psychiatry, 19(1), 152. |
| [16] | Du N., Yu K., Ye Y., & Chen S. (2017). Validity study of Patient Health Questionnaire-9 items for Internet screening in depression among Chinese university students. Asia- Pacific Psychiatry, 9(3), e12266. |
| [17] | Du X., Witthöft M., Zhang T., Shi C., & Ren Z. (2023). Interpretation bias in health anxiety: A systematic review and meta-analysis. Psychological Medicine, 53(1), 34-45. |
| [18] |
Eilenberg T., Hoffmann D., Jensen J. S., & Frostholm L. (2017). Intervening variables in group-based acceptance & commitment therapy for severe health anxiety. Behaviour Research and Therapy, 92, 24-31.
doi: S0005-7967(17)30016-5 pmid: 28196772 |
| [19] |
Falkenstein M., Kelley K., Dattolico D., Kuckertz J., Bezahler A., Krompinger J., Webb C., & Beard C. (2022). Feasibility and acceptability of cognitive bias modification for interpretation as an adjunctive treatment for OCD and related disorders: A pilot randomized controlled trial. Behavior Therapy, 53(2), 294-309.
doi: 10.1016/j.beth.2021.09.002 pmid: 35227405 |
| [20] | Fodor L. A., Georgescu R., Cuijpers P., Szamoskozi Ş., David D., Furukawa T. A., & Cristea I. A. (2020). Efficacy of cognitive bias modification interventions in anxiety and depressive disorders: A systematic review and network meta-analysis. The Lancet Psychiatry, 7(6), 506-514. |
| [21] | Frazier P. A., Tix A. P., & Barron K. E. (2004). Testing moderator and mediator effects in counseling psychology research. Journal of Counseling Psychology, 51(1), 115-134. |
| [22] | Gellatly R., & Beck A. T. (2016). Catastrophic thinking: A transdiagnostic process across psychiatric disorders. Cognitive Therapy and Research, 40(4), 441-452. |
| [23] |
Gong Y., Zhou H., Zhang Y., Zhu X., Wang X., Shen B., Xian J., & Ding Y. (2021). Validation of the 7-item Generalized Anxiety Disorder scale (GAD-7) as a screening tool for anxiety among pregnant Chinese women. Journal of Affective Disorders, 282, 98-103.
doi: 10.1016/j.jad.2020.12.129 pmid: 33401129 |
| [24] | Hedman E., Axelsson E., Gorling A., Ritzman C., Ronnheden M., El Alaoui S., ... Ljótsson B. (2014). Internet-delivered exposure-based cognitive-behavioural therapy and behavioural stress management for severe health anxiety: Randomised controlled trial. The British Journal of Psychiatry, 205(4), 307-314. |
| [25] | Hedman-Lagerlöf E., Tyrer P., Hague J., & Tyrer H. (2019). Health anxiety. BMJ, 364, l774. |
| [26] |
Helmich M. A., Wichers M., Olthof M., Strunk G., Aas B., Aichhorn W., Schiepek G., & Snippe E. (2020). Sudden gains in day-to-day change: Revealing nonlinear patterns of individual improvement in depression. Journal of Consulting and Clinical Psychology, 88(2), 119-127.
doi: 10.1037/ccp0000469 pmid: 31894994 |
| [27] |
Hirsch C. R., Krahé C., Whyte J., Krzyzanowski H., Meeten F., Norton S., & Mathews A. (2021). Internet-delivered interpretation training reduces worry and anxiety in individuals with generalized anxiety disorder: A randomized controlled experiment. Journal of Consulting and Clinical Psychology, 89(7), 575-589.
doi: 10.1037/ccp0000660 pmid: 34383532 |
| [28] | Hirsch C. R., Meeten F., Krahé C., & Reeder C. (2016). Resolving ambiguity in emotional disorders: The nature and role of interpretation biases. Annual Review of Clinical Psychology, 12(1), 281-305. |
| [29] | Hoffmann D., Rask C. U., Hedman-Lagerlöf E., Jensen J. S., & Frostholm L. (2021). Efficacy of internet-delivered acceptance and commitment therapy for severe health anxiety: Results from a randomized, controlled trial. Psychological Medicine, 51(15), 2685-2695. |
| [30] | Hu L., & Bentler P. M. (1998). Fit indices in covariance structure modeling: Sensitivity to underparameterized model misspecification. Psychological Methods, 3(4), 424-453. |
| [31] | Hu L., & Bentler P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 1-55. |
| [32] | Jalloh M. F., Li W., Bunnell R. E., Ethier K. A., O' Leary A., Hageman K. M., ... Redd J. T. (2018). Impact of Ebola experiences and risk perceptions on mental health in Sierra Leone, July 2015. BMJ Global Health, 3(2), e000471. |
| [33] | Ji J. L., Baee S., Zhang D., Calicho-Mamani C. P., Meyer M. J., Funk D., … Teachman B. A. (2021). Multi-session online interpretation bias training for anxiety in a community sample. Behaviour Research and Therapy, 142, 103864. |
| [34] |
Jones E. B., & Sharpe L. (2017). Cognitive bias modification: A review of meta-analyses. Journal of Affective Disorders, 223, 175-183.
doi: S0165-0327(17)31096-0 pmid: 28759865 |
| [35] | Kerstner T., Witthöft M., Mier D., Diener C., Rist F., & Bailer J. (2015). A diary-based modification of symptom attributions in pathological health anxiety: Effects on symptom report and cognitive biases. Journal of Consulting and Clinical Psychology, 83(3), 578-589. |
| [36] | Kisbu-Sakarya Y., Mackinnon D. P., & Aiken L. S. (2013). A monte carlo comparison study of the power of the analysis of covariance, simple difference, and residual change scores in testing two-wave data. Educational & Psychological Measurement, 73(1), 47-62. |
| [37] | Krebs G., Pil V., Grant S., Esposti M. D., Montgomery P., & Lau J. Y. F. (2018). Research review: Cognitive bias modification of interpretations in youth and its effect on anxiety: A meta-analysis. Journal of Child Psychology and Psychiatry, 59(8), 831-844. |
| [38] | Kroenke K., & Spitzer R. L. (2002). The PHQ-9: A new depression diagnostic and severity measure. Psychiatric Annals, 32(9), 509-515. |
| [39] |
Lau J. Y. F., Badaoui M., Meehan A. J., Heathcote L. C., Barker E. D., & Rimes K. A. (2020). Assessing the content specificity of interpretation biases in community adolescents with persistent and interfering pain. Pain, 161(2), 319-327.
doi: 10.1097/j.pain.0000000000001723 pmid: 31634340 |
| [40] | Liao S.-C., & Huang W.-L. (2021). Psychometric properties of the Chinese version of the cognitions about body and health questionnaire. Neuropsychiatric Disease and Treatment, 17, 1135-1144. |
| [41] | Liu B., & Li X. (2018). Cognitive bias modification of interpretation for social anxiety: A "bottom-up" intervention? Advances in Psychological Science, 26(5), 859-871. |
|
[刘冰茜, 李雪冰. (2018). 解释偏向矫正: “自下而上”地改变社交焦虑个体的解释偏向? 心理科学进展, 26(5), 859-871.]
doi: 10.3724/SP.J.1042.2018.00859 |
|
| [42] |
Longmore R. J., & Worrell M. (2007). Do we need to challenge thoughts in cognitive behavior therapy? Clinical Psychology Review, 27(2), 173-187.
pmid: 17157970 |
| [43] | Luo J., Wang P., Li Z., Cao W., Liu H., Meng L., & Sun J. (2021). Health anxiety and its correlates in the general Chinese population during the COVID-19 epidemic. Frontiers in Psychiatry, 12, 743409. |
| [44] | MacLeod C., & Mathews A. (2012). Cognitive bias modification approaches to anxiety. Annual Review of Clinical Psychology, 8(1), 189-217. |
| [45] | Mahase E. (2020). China coronavirus: Who declares international emergency as death toll exceeds 200. British Medical Journal, 368, m408. |
| [46] | Main A., Zhou Q., Ma Y., Luecken L. J., & Liu X. (2011). Relations of SARS-related stressors and coping to Chinese college students’ psychological adjustment during the 2003 Beijing SARS epidemic. Journal of Counseling Psychology, 58(3), 410-423. |
| [47] |
Mathews A., & Mackintosh B. (2000). Induced emotional interpretation bias and anxiety. Journal of Abnormal Psychology, 109(4), 602-615.
pmid: 11195984 |
| [48] |
Mcmanus F., Surawy C., Muse K., Vazquez-Montes M., & Williams J. M. G. (2012). A randomized clinical trial of mindfulness-based cognitive therapy versus unrestricted services for health anxiety (hypochondriasis). Journal of Consulting and Clinical Psychology, 80(5), 817-828.
pmid: 22708977 |
| [49] | Menne-Lothmann C., Viechtbauer W., Höhn P., Kasanova Z., Haller S. P., Drukker M., ... Lau J. Y. F. (2014). How to boost positive interpretations? A meta-analysis of the effectiveness of cognitive bias modification for interpretation. PLoS ONE, 9(6), e100925. |
| [50] | Midi H., & Bagheri A. (2010). Robust multicollinearity diagnostic measure in collinear data set. In Proceedings of the 4th international conference on applied mathematics, simulation, modeling (pp. 138-142). World Scientific and Engineering Academy and Society. |
| [51] |
Mobini S., Mackintosh B., Illingworth J., Gega L., Langdon P., & Hoppitt L. (2014). Effects of standard and explicit cognitive bias modification and computer-administered cognitive-behaviour therapy on cognitive biases and social anxiety. Journal of Behavior Therapy and Experimental Psychiatry, 45(2), 272-279.
doi: 10.1016/j.jbtep.2013.12.002 pmid: 24412966 |
| [52] |
Morriss R., Patel S., Malins S., Guo B., Higton F., James M., ... Tyrer H. (2019). Clinical and economic outcomes of remotely delivered cognitive behaviour therapy versus treatment as usual for repeat unscheduled care users with severe health anxiety: A multicentre randomised controlled trial. BMC Medicine, 17(1), 16.
doi: 10.1186/s12916-019-1253-5 pmid: 30670044 |
| [53] | Nieto I., & Vazquez C. (2021). Disentangling the mediating role of modifying interpretation bias on emotional distress using a novel cognitive bias modification program. Journal of Anxiety Disorders, 83, 102459. |
| [54] |
Olatunji B. O., Kauffman B. Y., Meltzer S., Davis M. L., Smits J. A. J., & Powers M. B. (2014). Cognitive- behavioral therapy for hypochondriasis/health anxiety: A meta-analysis of treatment outcome and moderators. Behaviour Research and Therapy, 58, 65-74.
doi: 10.1016/j.brat.2014.05.002 pmid: 24954212 |
| [55] |
Ren Z., Lai L., Yu X., Li S., Ruan Y., Zhao L. (2016). Meta-analysis on CBM for anxiety disorder: Effect sizes, moderators and mediation. Advances in Psychological Science, 24(11), 1690-1711.
doi: 10.3724/SP.J.1042.2016.01690 |
| [任志洪, 赖丽足, 余香莲, 李松蔚, 阮怡君, 赵陵波. (2016). 焦虑障碍的认知偏向矫正元分析: 效果量, 影响因素及中介检验. 心理科学进展, 24(11), 1690-1711.] | |
| [56] |
Ren Z., Li X., Zhao L., Yu X., Li Z., Lai L., Yuan Y., & Jiang G. (2016). Effectiveness and mechanism of internet-based self-help intervention for depression: The Chinese version of MoodGYM. Acta Psychologica Sinica, 48(7), 818-832.
doi: 10.3724/SP.J.1041.2016.00818 |
| [任志洪, 李献云, 赵陵波, 余香莲, 李政汉, 赖丽足, 阮怡君, 江光荣. (2016). 抑郁症网络化自助干预的效果及作用机制——以汉化moodgym为例. 心理学报, 48(7), 818-832.] | |
| [57] |
Ren Z., Zhao C., Bian C., Zhu W., Jiang G., Zhu Z. (2019). Mechanisms of the Acceptance and Commitment Therapy: A meta-analytic structural equation model. Acta Psychologica Sinica, 51(6), 662-676.
doi: 10.3724/SP.J.1041.2019.00662 |
|
[任志洪, 赵春晓, 卞诚, 朱文臻, 江光荣, 祝卓宏. (2019). 接纳承诺疗法的作用机制——基于元分析结构方程模型. 心理学报, 51(6), 662-676.]
doi: 10.3724/SP.J.1041.2019.00662 |
|
| [58] | Ren Z., Zhao Z., Yu X., Zhang L., & Li X. (2021). Modification of hostile interpretation bias and self-reported aggression in juvenile delinquents: A randomized controlled trial. International Journal of Clinical and Health Psychology, 21(2), 100226. |
| [59] |
Rief W., Hiller W., & Margraf J. (1998). Cognitive aspects of hypochondriasis and the somatization syndrome. Journal of Abnormal Psychology, 107(4), 587-595.
pmid: 9830246 |
| [60] | Rios K., Sosa N., & Osborn H. (2018). An experimental approach to Intergroup Threat Theory: Manipulations, moderators, and consequences of realistic vs. symbolic threat. European Review of Social Psychology, 29(1), 212-255. |
| [61] | Rogosa D. R., Brandt D., & Zimowski M. (1982). A growth curve approach to the measurement of change. Psychological Bulletin, 92(3), 726-748. |
| [62] |
Rozenman M., Gonzalez A., Logan C., & Goger P. (2020). Cognitive bias modification for threat interpretations: Impact on anxiety symptoms and stress reactivity. Depression and Anxiety, 37(5), 438-448.
doi: 10.1002/da.23018 pmid: 32301579 |
| [63] |
Salemink E., van den Hout M., & Kindt M. (2010). How does cognitive bias modification affect anxiety? Mediation analyses and experimental data. Behavioural and Cognitive Psychotherapy, 38(1), 59-66.
doi: 10.1017/S1352465809990543 pmid: 19995465 |
| [64] |
Salkovskis P. M., & Warwick H. M. C. (1986). Morbid preoccupations, health anxiety and reassurance: A cognitive-behavioural approach to hypochondriasis. Behaviour Research and Therapy, 24(5), 597-602.
doi: 10.1016/0005-7967(86)90041-0 pmid: 3753387 |
| [65] |
Salkovskis P. M., Rimes K. A., Warwick H. M. C., & Clark D. M. (2002). The health anxiety inventory: Development and validation of scales for the measurement of health anxiety and hypochondriasis. Psychological Medicine, 32(5), 843-853.
doi: 10.1017/s0033291702005822 pmid: 12171378 |
| [66] | Schulz K. F., Altman D. G., Moher D., & CONSORT Group. (2010). CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMJ, 340, c332-c332. |
| [67] | Selig J. P., & Preacher K. J. (2009). Mediation models for longitudinal data in developmental research. Research in Human Development, 6(2-3), 144-164. |
| [68] |
Sørensen P., Birket-Smith M., Wattar U., Buemann I., & Salkovskis P. (2011). A randomized clinical trial of cognitive behavioural therapy versus short-term psychodynamic psychotherapy versus no intervention for patients with hypochondriasis. Psychological Medicine, 41(2), 431-441.
doi: 10.1017/S0033291710000292 pmid: 20380779 |
| [69] |
Spitzer R. L., Kroenke K., Williams J. B. W., & Löwe B. (2006). A brief measure for assessing generalized anxiety disorder: The GAD-7. Archives of Internal Medicine, 166(10), 1092-1097.
doi: 10.1001/archinte.166.10.1092 pmid: 16717171 |
| [70] | Taylor S., & Asmundson G. J. G. (2004). Treating health anxiety: A cognitive-behavioral approach. Guilford Press. |
| [71] | Tolgou T., Rohrmann S., Stockhausen C., Krampen D., Warnecke I., & Reiss N. (2018). Physiological and psychological effects of imagery techniques on health anxiety. Psychophysiology, 55(2), e12984. |
| [72] | Tyrer P. (2020). COVID-19 health anxiety. World Psychiatry, 19(3), 307-308. |
| [73] | Tyrer P., Cooper S., Salkovskis P., Tyrer H., Crawford M., Byford S., ... Barrett B. (2014). Clinical and cost- effectiveness of cognitive behaviour therapy for health anxiety in medical patients: A multicentre randomised controlled trial. The Lancet, 383(9913), 219-225. |
| [74] |
van Teffelen M., Lobbestael J., Voncken M., Cougle J., & Peeters F. (2021). Interpretation bias modification for hostility: A randomized clinical trial. Journal of Consulting and Clinical Psychology, 89(5), 421-434.
doi: 10.1037/ccp0000651 pmid: 34124926 |
| [75] |
Visser S., & Bouman T. K. (2001). The treatment of hypochondriasis: Exposure plus response prevention vs cognitive therapy. Behaviour Research and Therapy, 39(4), 423-442.
pmid: 11280341 |
| [76] | von Soest T., & Hagtvet K. A. (2011). Mediation analysis in a latent growth curve modeling framework. Structural Equation Modeling, 18(2), 289-314. |
| [77] |
Walker J., Vincent N., Furer P., Cox B., & Kevin Kjernisted. (1999). Treatment preference in hypochondriasis. Journal of Behavior Therapy and Experimental Psychiatry, 30(4), 251-258.
pmid: 10759322 |
| [78] |
Weck F., Gropalis M., Hiller W., & Bleichhardt G. (2015). Effectiveness of cognitive-behavioral group therapy for patients with hypochondriasis (health anxiety). Journal of Anxiety Disorders, 30, 1-7.
doi: 10.1016/j.janxdis.2014.12.012 pmid: 25589453 |
| [79] |
Weck F., Neng J. M. B., Richtberg S., Jakob M., & Stangier U. (2015). Cognitive therapy versus exposure therapy for hypochondriasis (health anxiety): A randomized controlled trial. Journal of Consulting and Clinical Psychology, 83(4), 665-676.
doi: 10.1037/ccp0000013 pmid: 25495359 |
| [80] |
Weck F., Neng J. M. B., Schwind J., & Höfling V. (2015). Exposure therapy changes dysfunctional evaluations of somatic symptoms in patients with hypochondriasis (health anxiety). A randomized controlled trial. Journal of Anxiety Disorders, 34, 1-7.
doi: 10.1016/j.janxdis.2015.05.008 pmid: 26093823 |
| [81] | Williams P. G. (2004). The psychopathology of self-assessed health: A cognitive approach to health anxiety and hypochondriasis. Cognitive Therapy and Research, 28(5), 629-644. |
| [82] | Woud M. L., Wittekind C. E., & Würtz F. (2022). Cognitive bias modification bei symptomen der posttraumatischen belastungsstörung. Verhaltenstherapie, 32(3), 139-147. |
| [83] | Yan Z., Witthöft M., Bailer J., Diener C., & Mier D. (2019). Scary symptoms? Functional magnetic resonance imaging evidence for symptom interpretation bias in pathological health anxiety. European Archives of Psychiatry and Clinical Neuroscience, 269(4), 195-207. |
| [84] |
Yang R., Cui L., Li F., Xiao J., Zhang Q., & Oei T. P. S. (2017). Effects of cognitive bias modification training via smartphones. Frontiers in Psychology, 8, 1370.
doi: 10.3389/fpsyg.2017.01370 pmid: 28855880 |
| [85] | Yuan Y., & Zhang Y. (2013). Health anxiety of patients with chronic disease and its influencing factors. In Psychology and Enhancement of Innovation Capability - Proceedings of the 16th National Academic Congress of Psychology (pp. 2263-2264). Nanjing, China: Chinese Psychological Society. |
| [袁勇贵, 张钰群. (2013). 慢性病患者的健康焦虑及其影响因素研究. 心理学与创新能力提升——第十六届全国心理学学术会议论文集 (pp. 2263-2264). 南京, 中国: 中国心理学会.] | |
| [86] | Zhang F., Huang C., Mao X., Hou T., Sun L., Zhou Y., & Deng G. (2021). Efficacy of the Chinese version interpretation bias modification training in an unselected sample: A randomized trial. PLOS ONE, 16(7), e0255224. |
| [87] |
Zhang Y., Liu R., Li G., Mao S., & Yuan Y. (2015). The reliability and validity of a Chinese-version short health anxiety inventory: An investigation of university students. Neuropsychiatric Disease and Treatment, 11, 1739-1747.
doi: 10.2147/NDT.S83501 pmid: 26213472 |
| [1] | 陆嘉琦, 李雨斯, 何贵兵. 双相障碍患者的风险决策偏好:来自三水平元分析的证据[J]. 心理学报, 2025, 57(1): 100-124. |
| [2] | 尹华站, 肖春花, 夏安妮, 袁中静, 崔晓冰, 李丹. 基本情绪对时距知觉的影响: 来自三水平元分析和网络元分析的证据[J]. 心理学报, 2024, 56(12): 1676-1690. |
| [3] | 吴政宇, 王飞, 王德文, 刘正奎. 高原之上的忧郁: 海拔高度与抑郁风险的关系[J]. 心理学报, 2024, 56(12): 1773-1787. |
| [4] | 王婷, 赵梁佛, 杨金朋, 张丹丹, 雷震. 分配意图与上行间接互惠:来自行为与ERP的证据[J]. 心理学报, 2024, 56(12): 1788-1799. |
| [5] | 邱义, 常香玉, 涂毅恒. 双靶点经颅直流电刺激调控短时和持续性疼痛:一项双盲、随机对照研究[J]. 心理学报, 2024, 56(10): 1313-1327. |
| [6] | 王彪, 王珍珍, 刘兴华. 融合中国诗词的线上自助正念干预的可行性及对参与者依从性的影响[J]. 心理学报, 2024, 56(8): 1110-1124. |
| [7] | 杨之旭, 彭海云, 辛素飞. 疫情后期青少年的抑郁和焦虑变迁趋势及其潜在因果:一项追踪研究[J]. 心理学报, 2024, 56(4): 482-496. |
| [8] | 孙启武, 王之焕, 任志洪, 于丽霞, 吴才智. 视频咨询不会削弱咨询效果:来自与线下面询比较的证据[J]. 心理学报, 2023, 55(11): 1845-1858. |
| [9] | 张文芸, 卓诗维, 郑倩倩, 关颖琳, 彭微微. 自闭特质对疼痛共情的影响:疼痛负性情绪和认知的中介作用[J]. 心理学报, 2023, 55(9): 1501-1517. |
| [10] | 陈诗韵, 屈笛扬, 卜禾, 梁凯欣, 张沛超, 迟新丽. 迷“网”的少年:网瘾风险青少年的症状演化*[J]. 心理学报, 2023, 55(9): 1465-1476. |
| [11] | 梅颖, 刘郡彤, 刘红红, 傅洋, 罗熙, 雷怡. 自悯写作对恐惧消退的促进作用[J]. 心理学报, 2023, 55(8): 1317-1329. |
| [12] | 王妹, 程思, 李宜伟, 李红, 张丹丹. 背外侧前额叶在安慰剂效应中的作用:社会情绪调节研究[J]. 心理学报, 2023, 55(7): 1063-1073. |
| [13] | 李彧, 位东涛, 邱江. 抑郁症的人格类型及其脑功能连接基础[J]. 心理学报, 2023, 55(5): 740-751. |
| [14] | 高可翔, 张岳瑶, 李思瑾, 袁加锦, 李红, 张丹丹. 腹内侧前额叶在内隐认知重评中的因果作用[J]. 心理学报, 2023, 55(2): 210-223. |
| [15] | 王文超, 原昊, 伍新春. 灾后中小学生创伤后应激障碍和抑郁症状的共存模式[J]. 心理学报, 2022, 54(12): 1503-1516. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||