ISSN 1671-3710
CN 11-4766/R
主办:中国科学院心理研究所
出版:科学出版社
CN 11-4766/R
主办:中国科学院心理研究所
出版:科学出版社
心理科学进展 ›› 2022, Vol. 30 ›› Issue (11): 2518-2528.doi: 10.3724/SP.J.1042.2022.02518 cstr: 32111.14.2022.02518
顾丽佳1, 宫文潇2, 张静3,4, 陈巍1,5( ), 郭建友6,7
), 郭建友6,7
收稿日期:2021-12-24
出版日期:2022-11-15
发布日期:2022-11-09
基金资助:
GU Lijia1, GONG Wenxiao2, ZHANG Jing3,4, CHEN Wei1,5(), GUO Jianyou6,7
Received:2021-12-24
Online:2022-11-15
Published:2022-11-09
摘要:
身体拥有感错觉以多通道的感官整合为基础, 包括视觉-触觉、视觉-本体感觉、触觉-本体感觉、视觉-内感受的整合等。来自实验室急性痛以及慢性痛的大量结果表明拥有感错觉可产生镇痛作用。身体部位尺寸大小、肢体透明度等相关影响因素也逐渐得到揭示。拥有感错觉影响疼痛的机制与身体表征的改变有关, 该过程可能涉及“身体网络”与“疼痛网络”间的连接, 其中后顶叶皮层可能有重要作用。未来研究应更为深入地探索拥有感错觉范式以考察不同因素对疼痛的影响; 在现有多感官整合的范式中重视内感受的作用; 考察拥有感错觉改变疼痛的认知神经机制; 区分急、慢性痛条件下以及不同慢性痛类型中拥有感错觉对疼痛的不同影响。
中图分类号:
顾丽佳, 宫文潇, 张静, 陈巍, 郭建友. (2022). 身体拥有感错觉对疼痛的影响及其作用机制. 心理科学进展 , 30(11), 2518-2528.
GU Lijia, GONG Wenxiao, ZHANG Jing, CHEN Wei, GUO Jianyou. (2022). The influence of body ownership illusion on pain and its potential mechanisms. Advances in Psychological Science, 30(11), 2518-2528.
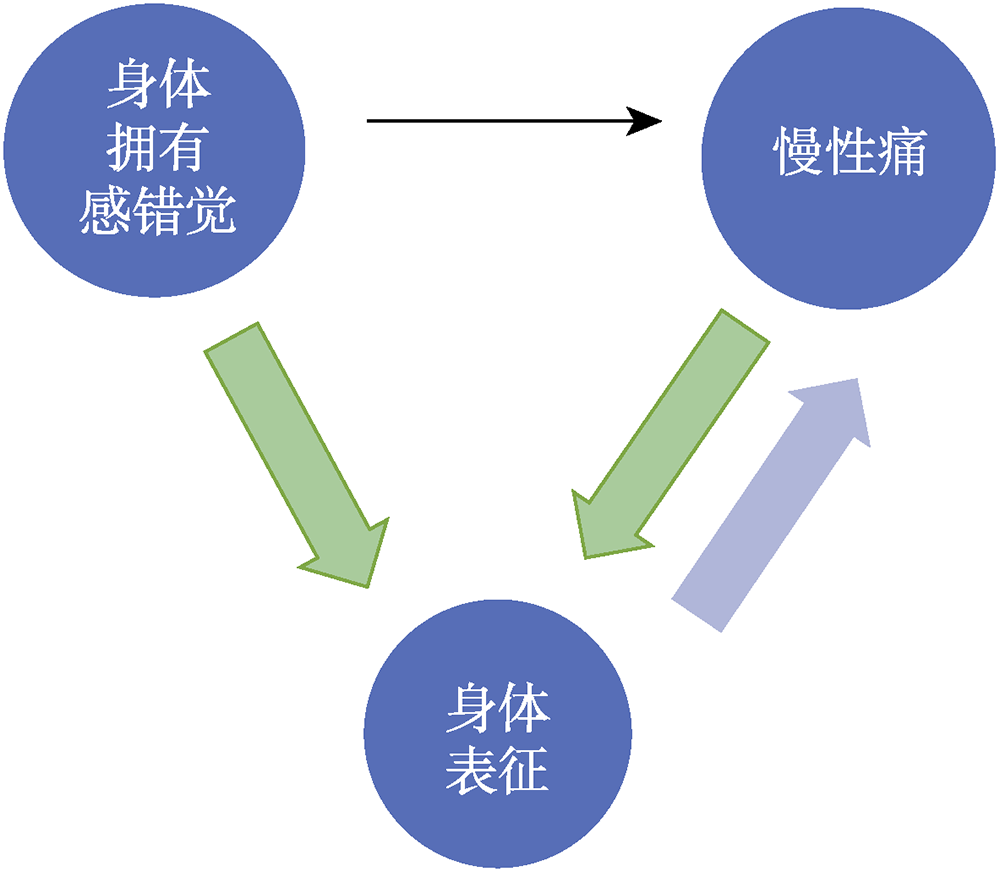
图1 身体拥有感错觉、身体表征与疼痛
| [1] |
Boesch, E., Bellan, V., Moseley, G. L., & Stanton, T. R. (2016). The effect of bodily illusions on clinical pain: A systematic review and meta-analysis. Pain, 157(3), 516-529.
doi: 10.1097/j.pain.0000000000000423 pmid: 26588692 |
| [2] |
Botvinick, M., & Cohen, J. (1998). Rubber hands ‘feel’ touch that eyes see. Nature, 391(6669), 756-756.
doi: 10.1038/35784 URL |
| [3] | Braun, N., Debener, S., Spychala, N., Bongartz, E., Sörös, P., Müller, H. H. O., & Philipsen, A. (2018). The senses of agency and ownership: A review. Frontiers in Psychology, 9, Article 535. |
| [4] |
Chancel, M., & Ehrsson, H. H. (2020). Which hand is mine? Discriminating body ownership perception in a two- alternative forced-choice task. Attention, Perception, & Psychophysics, 82(8), 4058-4083.
doi: 10.3758/s13414-020-02107-x URL |
| [5] |
Coleshill, M. J., George, D. N., & Mazzoni, G. (2017). Placebo analgesia from a rubber hand. Journal of Pain, 18(9), 1067-1077.
doi: S1526-5900(17)30558-8 pmid: 28455248 |
| [6] | Connell, L., Lynott, D., & Banks, B. (2018). Interoception: The forgotten modality in perceptual grounding of abstract and concrete concepts. Philosophical Transactions of the Royal Society B: Biological Sciences, 373(1752), Article 20170143. |
| [7] |
Cordier, L., Fuchs, X., Herpertz, S., Trojan, J., & Diers, M. (2020). Synchronous stimulation with light and heat induces body ownership and reduces pain perception. Journal of Pain, 21(5-6), 700-707.
doi: S1526-5900(19)30846-6 pmid: 31698132 |
| [8] |
Craig, A. D. (2002). How do you feel? Interoception: The sense of the physiological condition of the body. Nature Reviews Neuroscience, 3(8), 655-666.
doi: 10.1038/nrn894 pmid: 12154366 |
| [9] |
Edwards, L., Inui, K., Ring, C., Wang, X., & Kakigi, R. (2008). Pain-related evoked potentials are modulated across the cardiac cycle. Pain, 137(3), 488-494.
doi: 10.1016/j.pain.2007.10.010 pmid: 18035494 |
| [10] | Ehrsson, H. H. (2007). The experimental induction of out-of-body experiences. Science, 317(5841), 1048. |
| [11] | Ehrsson, H. H. (2020). Multisensory processes in body ownership. In K. Sathian & V. S. Ramachandran (Eds.), Multisensory perception: From laboratory to clinic (pp. 179-200). Elsevier. |
| [12] |
Ehrsson, H. H., Holmes, N. P., & Passingham, R. E. (2005). Touching a rubber hand: Feeling of body ownership is associated with activity in multisensory brain areas. Journal of Neuroscience, 25(45), 10564-10573.
doi: 10.1523/JNEUROSCI.0800-05.2005 pmid: 16280594 |
| [13] |
Ehrsson, H. H., Wiech, K., Weiskopf, N., Dolan, R. J., & Passingham, R. E. (2007). Threatening a rubber hand that you feel is yours elicits a cortical anxiety response. Proceedings of the National Academy of Sciences of the United States of America, 104(23), 9828-9833.
pmid: 17517605 |
| [14] | Fang, W., Zhang, R., Zhao, Y., Wang, L., & Zhou, Y.-D. (2019). Attenuation of pain perception induced by the rubber hand illusion. Frontiers in Neuroscience, 13, Article 261. |
| [15] |
Foell, J., Bekrater-Bodmann, R., Diers, M., & Flor, H. (2014). Mirror therapy for phantom limb pain: Brain changes and the role of body representation. European Journal of Pain, 18(5), 729-739.
doi: 10.1002/j.1532-2149.2013.00433.x pmid: 24327313 |
| [16] | Gallagher, M., Colzi, C., & Sedda, A. (2021). Dissociation of proprioceptive drift and feelings of ownership in the somatic rubber hand illusion. Acta Psychologica, 212, Article 103192. |
| [17] |
Gallagher, S. (2000). Philosophical conceptions of the self: Implications for cognitive science. Trends in Cognitive Sciences, 4(1), 14-21.
pmid: 10637618 |
| [18] |
Gilpin, H. R., Moseley, G. L., Stanton, T. R., & Newport, R. (2015). Evidence for distorted mental representation of the hand in osteoarthritis. Rheumatology, 54(4), 678-682.
doi: 10.1093/rheumatology/keu367 pmid: 25246638 |
| [19] |
Hänsel, A., Lenggenhager, B., von Känel, R., Curatolo, M., & Blanke, O. (2011). Seeing and identifying with a virtual body decreases pain perception. European Journal of Pain, 15(8), 874-879.
doi: 10.1016/j.ejpain.2011.03.013 pmid: 21570328 |
| [20] |
Hegedues, G., Darnai, G., Szolcsanyi, T., Feldmann, A., Janszky, J., & Kallai, J. (2014). The rubber hand illusion increases heat pain threshold. European Journal of Pain, 18(8), 1173-1181.
doi: 10.1002/j.1532-2149.2014.00466.x pmid: 24590760 |
| [21] | Henderson, L. A., di Pietro, F., Youssef, A. M., Lee, S., Tam, S., Akhter, R., Mills, E. P., Murray, G. M., Peck, C. C., & Macey, P. M. (2020). Effect of expectation on pain processing: A psychophysics and functional MRI analysis. Frontiers in Neuroscience, 14, Article 6. |
| [22] | Kalckert, A., & Ehrsson, H. H. (2012). Moving a rubber hand that feels like your own: A dissociation of ownership and agency. Frontiers in Human Neuroscience, 6, Article 40. |
| [23] |
Kalckert, A., & Ehrsson, H. H. (2014). The moving rubber hand illusion revisited: Comparing movements and visuotactile stimulation to induce illusory ownership. Consciousness and Cognition, 26, 117-132.
doi: 10.1016/j.concog.2014.02.003 pmid: 24705182 |
| [24] | Keenaghan, S., Bowles, L., Crawfurd, G., Thurlbeck, S., Kentridge, R. W., & Cowie, D. (2020). My body until proven otherwise: Exploring the time course of the full body illusion. Consciousness and Cognition, 78, Article 102882. |
| [25] |
Kim, D., Woo, C.-W., & Kim, S.-G. (2021). Neural mechanisms of pain relief through paying attention to painful stimuli. Pain, 163(6), 1130-1138.
doi: 10.1097/j.pain.0000000000002464 pmid: 34433768 |
| [26] |
Legrain, V., Iannetti, G. D., Plaghki, L., & Mouraux, A. (2011). The pain matrix reloaded: A salience detection system for the body. Progress in Neurobiology, 93(1), 111-124.
doi: 10.1016/j.pneurobio.2010.10.005 pmid: 21040755 |
| [27] |
Lloyd, D. M. (2007). Spatial limits on referred touch to an alien limb may reflect boundaries of visuo-tactile peripersonal space surrounding the hand. Brain and Cognition, 64(1), 104-109.
pmid: 17118503 |
| [28] |
Longo, M. R., Betti, V., Aglioti, S. M., & Haggard, P. (2009). Visually induced analgesia: Seeing the body reduces pain. Journal of Neuroscience, 29(39), 12125-12130.
doi: 10.1523/JNEUROSCI.3072-09.2009 pmid: 19793970 |
| [29] |
Longo, M. R., Iannetti, G. D., Mancini, F., Driver, J., & Haggard, P. (2012). Linking pain and the body: Neural correlates of visually induced analgesia. Journal of Neuroscience, 32(8), 2601-2607.
doi: 10.1523/JNEUROSCI.4031-11.2012 pmid: 22357844 |
| [30] |
Maihöfner, C., Handwerker, H. O., Neundörfer, B., & Birklein, F. (2003). Patterns of cortical reorganization in complex regional pain syndrome. Neurology, 61(12), 1707-1715.
pmid: 14694034 |
| [31] |
Mancini, F., Longo, M. R., Canzoneri, E., Vallar, G., & Haggard, P. (2013). Changes in cortical oscillations linked to multisensory modulation of nociception. European Journal of Neuroscience, 37(5), 768-776.
doi: 10.1111/ejn.12080 pmid: 23216684 |
| [32] |
Mancini, F., Longo, M. R., Kammers, M. P., & Haggard, P. (2011). Visual distortion of body size modulates pain perception. Psychological Science, 22(3), 325-330.
doi: 10.1177/0956797611398496 pmid: 21303990 |
| [33] | Martínez, E., Aira, Z., Buesa, I., Aizpurua, I., Rada, D., & Azkue, J. J. (2018). Embodied pain in fibromyalgia: Disturbed somatorepresentations and increased plasticity of the body schema. PloS One, 13(4), Article e0194534. |
| [34] | Martini, M., Kilteni, K., Maselli, A., & Sanchez-Vives, M. V. (2015). The body fades away: Investigating the effects of transparency of an embodied virtual body on pain threshold and body ownership. Scientific Reports, 5, Article13948. |
| [35] | Martini, M., Perez-Marcos, D., & Sanchez-Vives, M. V. (2013). What color is my arm? Changes in skin color of an embodied virtual arm modulates pain threshold. Frontiers in Human Neuroscience, 7, Article 438. |
| [36] |
Martini, M., Perez-Marcos, D., & Sanchez-Vives, M. V. (2014). Modulation of pain threshold by virtual body ownership. European Journal of Pain, 18(7), 1040-1048.
doi: 10.1002/j.1532-2149.2014.00451.x pmid: 24449513 |
| [37] | Maselli, A., & Slater, M. (2013). The building blocks of the full body ownership illusion. Frontiers in Human Neuroscience, 7, Article 83. |
| [38] |
Matamala-Gomez, M., Diaz Gonzalez, A. M., Slater, M., & Sanchez-Vives, M. V. (2019a). Decreasing pain ratings in chronic arm pain through changing a virtual body: Different strategies for different pain types. Journal of Pain, 20(6), 685-697.
doi: 10.1016/j.jpain.2018.12.001 URL |
| [39] | Matamala-Gomez, M., Donegan, T., Bottiroli, S., Sandrini, G., Sanchez-Vives, M. V., & Tassorelli, C. (2019b). Immersive virtual reality and virtual embodiment for pain relief. Frontiers in Human Neuroscience, 13, Article 279. |
| [40] | Matamala-Gomez, M., Malighetti, C., Cipresso, P., Pedroli, E., Realdon, O., Mantovani, F., & Riva, G. (2020). Changing body representation through full body ownership illusions might foster motor rehabilitation outcome in patients with stroke. Frontiers in Psychology, 11, Article 1962. |
| [41] | Mohan, R., Jensen, K. B., Petkova, V. I., Dey, A., Barnsley, N., Ingvar, M., McAuley, J. H., Moseley, G. L., & Ehrsson, H. H. (2012). No pain relief with the rubber hand illusion. PloS One, 7(12), Article e52400. |
| [42] |
Moseley, G. L. (2007). Using visual illusion to reduce at- level neuropathic pain in paraplegia. Pain, 130(3), 294-298.
doi: 10.1016/j.pain.2007.01.007 URL |
| [43] |
Moseley, G. L., Gallace, A., & Spence, C. (2012). Bodily illusions in health and disease: Physiological and clinical perspectives and the concept of a cortical 'body matrix'. Neuroscience and Biobehavioral Reviews, 36(1), 34-46.
doi: 10.1016/j.neubiorev.2011.03.013 pmid: 21477616 |
| [44] | Moseley, G. L., Parsons, T. J., & Spence, C. (2008). Visual distortion of a limb modulates the pain and swelling evoked by movement. Current Biology, 18(22), R1047- R1048. |
| [45] |
Ng, S. K., Urquhart, D. M., Fitzgerald, P. B., Kirkovski, M., Cicuttini, F. M., Maller, J. J., Enticott, P. G., Rossell, S. L., & Fitzgibbon, B. M. (2021). Neural activity during cognitive reappraisal in chronic low back pain: A preliminary study. Scandinavian Journal of Pain, 21(3), 586-596.
doi: 10.1515/sjpain-2020-0146 pmid: 33838093 |
| [46] |
Nierula, B., Martini, M., Matamala-Gomez, M., Slater, M., & Sanchez-Vives, M. V. (2017). Seeing an embodied virtual hand is analgesic contingent on colocation. Journal of Pain, 18(6), 645-655.
doi: S1526-5900(17)30017-2 pmid: 28108385 |
| [47] |
Packham, T. L., Wainio, K., & Wong, M.-K. (2020). Persons with complex regional pain syndrome renegotiate social roles and intimacy: A qualitative study. Pain Medicine, 21(2), 239-246.
doi: 10.1093/pm/pnz173 pmid: 31504892 |
| [48] |
Pamment, J., & Aspell, J. E. (2017). Putting pain out of mind with an "out of body' illusion. European Journal of Pain, 21(2), 334-342.
doi: 10.1002/ejp.927 pmid: 27509229 |
| [49] |
Pazzaglia, M., Haggard, P., Scivoletto, G., Molinari, M., & Lenggenhager, B. (2016). Pain and somatic sensation are transiently normalized by illusory body ownership in a patient with spinal cord injury. Restorative Neurology and Neuroscience, 34(4), 603-613.
doi: 10.3233/RNN-150611 pmid: 27080071 |
| [50] |
Peltz, E., Seifert, F., Lanz, S., Müller, R., & Maihöfner, C. (2011). Impaired hand size estimation in CRPS. Journal of Pain, 12(10), 1095-1101.
doi: 10.1016/j.jpain.2011.05.001 pmid: 21741321 |
| [51] |
Pozeg, P., Palluel, E., Ronchi, R., Solcà, M., Al-Khodairy, A.-W., Jordan, X., Kassouha, A., & Blanke, O. (2017). Virtual reality improves embodiment and neuropathic pain caused by spinal cord injury. Neurology, 89(18), 1894-1903.
doi: 10.1212/WNL.0000000000004585 pmid: 28986411 |
| [52] | Preston, C., Gilpin, H. R., & Newport, R. (2020). An exploratory investigation into the longevity of pain reduction following multisensory illusions designed to alter body perception. Musculoskeletal Science and Practice, 45, Article 102080. |
| [53] |
Pyasik, M., Salatino, A., & Pia, L. (2019). Do movements contribute to sense of body ownership? Rubber hand illusion in expert pianists. Psychological Research, 83(1), 185-195.
doi: 10.1007/s00426-018-1137-x pmid: 30560294 |
| [54] | Pyasik, M., Tieri, G., & Pia, L. (2020). Visual appearance of the virtual hand affects embodiment in the virtual hand illusion. Scientific Reports, 10(1), Article 5412. |
| [55] |
Raja, S. N., Carr, D. B., Cohen, M., Finnerup, N. B., Flor, H., Gibson, S., … Vader, K. (2020). The revised International Association for the Study of Pain definition of pain: Concepts, challenges, and compromises. Pain, 161(9), 1976-1982.
doi: 10.1097/j.pain.0000000000001939 URL |
| [56] |
Ramachandran, V. S., Brang, D., & McGeoch, P. D. (2009). Size reduction using mirror visual feedback (MVF) reduces phantom pain. Neurocase, 15(5), 357-360.
doi: 10.1080/13554790903081767 pmid: 19657972 |
| [57] | Ramachandran, V. S., & Rogers-Ramachandran, D. (1996). Synaesthesia in phantom limbs induced with mirrors. Proceedings of the Royal Society of London Series B: Biological Sciences, 263(1369), 377-386. |
| [58] |
Riva, G. (2018). The neuroscience of body memory: From the self through the space to the others. Cortex, 104, 241-260.
doi: S0010-9452(17)30238-1 pmid: 28826604 |
| [59] |
Romano, D., Llobera, J., & Blanke, O. (2016). Size and viewpoint of an embodied virtual body affect the processing of painful stimuli. Journal of Pain, 17(3), 350-358.
doi: 10.1016/j.jpain.2015.11.005 URL |
| [60] |
Romano, D., Pfeiffer, C., Maravita, A., & Blanke, O. (2014). Illusory self-identification with an avatar reduces arousal responses to painful stimuli. Behavioural Brain Research, 261, 275-281.
doi: 10.1016/j.bbr.2013.12.049 pmid: 24412686 |
| [61] |
Schmalzl, L., Ragnö, C., & Ehrsson, H. H. (2013). An alternative to traditional mirror therapy: Illusory touch can reduce phantom pain when illusory movement does not. Clinical Journal of Pain, 29(10), 10-18.
doi: 10.1097/AJP.0b013e3182850573 pmid: 23446074 |
| [62] |
Siedlecka, M., Spychala, N., Lukowska, M., Wiercioch, K., & Wierzchoń, M. (2018). Rubber hand illusion increases pain caused by electric stimuli. Journal of Pain, 19(1), 35-45.
doi: S1526-5900(17)30685-5 pmid: 28864079 |
| [63] | Solcà, M., Ronchi, R., Bello-Ruiz, J., Schmidlin, T., Herbelin, B., Luthi, F., … Blanke, O. (2018). Heartbeat- enhanced immersive virtual reality to treat complex regional pain syndrome. Neurology, 91(5), E479-E489. |
| [64] |
Soler, M. D., Kumru, H., Pelayo, R., Vidal, J., Tormos, J. M., Fregni, F., Navarro, X., & Pascual-Leone, A. (2010). Effectiveness of transcranial direct current stimulation and visual illusion on neuropathic pain in spinal cord injury. Brain, 133(9), 2565-2577.
doi: 10.1093/brain/awq184 pmid: 20685806 |
| [65] | Stanton, T. R., Gilpin, H. R., Edwards, L., Moseley, G. L., & Newport, R. (2018). Illusory resizing of the painful knee is analgesic in symptomatic knee osteoarthritis. PeerJ, 6, Article e5206. |
| [66] |
Suzuki, K., Garfinkel, S. N., Critchley, H. D., & Seth, A. K. (2013). Multisensory integration across exteroceptive and interoceptive domains modulates self-experience in the rubber-hand illusion. Neuropsychologia, 51(13), 2909-2917.
doi: 10.1016/j.neuropsychologia.2013.08.014 pmid: 23993906 |
| [67] |
Taylor, V. A., Chang, L. K., Rainville, P., & Roy, M. (2017). Learned expectations and uncertainty facilitate pain during classical conditioning. Pain, 158(8), 1528-1537.
doi: 10.1097/j.pain.0000000000000948 pmid: 28715353 |
| [68] |
Ten Brink, A. F., & Bultitude, J. H. (2021). Predictors of self- reported neglect-like symptoms and involuntary movements in complex regional pain syndrome compared to other chronic limb pain conditions. Pain Medicine, 22(10), 2337-2349.
doi: 10.1093/pm/pnab226 URL |
| [69] | Trojan, J., Fuchs, X., Speth, S.-L., & Diers, M. (2018). The rubber hand illusion induced by visual-thermal stimulation. Scientific Reports, 8(1), Article 12417. |
| [70] |
Tsakiris, M. (2010). My body in the brain: A neurocognitive model of body-ownership. Neuropsychologia, 48(3), 703-712.
doi: 10.1016/j.neuropsychologia.2009.09.034 pmid: 19819247 |
| [71] |
Tsakiris, M., & Haggard, P. (2005). The rubber hand illusion revisited: Visuotactile integration and self-attribution. Journal of Experimental Psychology-Human Perception and Performance, 31(1), 80-91.
pmid: 15709864 |
| [72] | Valenzuela-Moguillansky, C. (2011). Role of body awareness. Journal of Consciousness Studies, 18(9-10), 110-142. |
| [73] | Valenzuela Moguillansky, C., O'Regan, J. K., & Petitmengin, C. (2013). Exploring the subjective experience of the "rubber hand" illusion. Frontiers in Human Neuroscience, 7, Article 659. |
| [74] | Viceconti, A., Camerone, E. M., Luzzi, D., Pentassuglia, D., Pardini, M., Ristori, D., Rossettini, G., Gallace, A., Longo, M. R., & Testa, M. (2020). Explicit and implicit own's body and space perception in painful musculoskeletal disorders and rheumatic diseases: A systematic scoping review. Frontiers in Human Neuroscience, 14, Article 83. |
| [1] | 丁颖, 汪紫滢, 李卫东. 抑郁症疼痛加工的行为特点及神经机制[J]. 心理科学进展, 2024, 32(8): 1315-1327. |
| [2] | 刘沛菡, 张火垠, 张旭凯, 李红, 雷怡. 急性疼痛与慢性疼痛对奖赏加工的影响及神经机制[J]. 心理科学进展, 2023, 31(3): 402-415. |
| [3] | 刘博, 程香娟, 岳衡, 包呼格吉乐图. 抑制功能在疼痛中的作用[J]. 心理科学进展, 2022, 30(6): 1253-1261. |
| [4] | 刘昕鹤, 王宁, 王锦琰, 罗非. 疼痛背景下时距知觉的变化[J]. 心理科学进展, 2020, 28(5): 766-777. |
| [5] | 张静, 陈巍. 身体拥有感及其可塑性:基于内外感受研究的视角[J]. 心理科学进展, 2020, 28(2): 305-315. |
| [6] | 赵佩琼, 陈巍, 张静, 平贤洁. 橡胶手错觉:拥有感研究的实验范式及其应用[J]. 心理科学进展, 2019, 27(1): 37-50. |
| [7] | 张静, 陈巍. 基于自我错觉的最小自我研究:具身建构论的立场[J]. 心理科学进展, 2018, 26(7): 1244-1252. |
| [8] | 竭 婧, 庄梦迪, 罗品超, 郑希付. 神经科学视角下的共情研究热点[J]. 心理科学进展, 2017, 25(11): 1922-1931. |
| [9] | 苏琳;杨周;Todd Jackson ;陈红;黄承志. 疼痛恐惧的形成及其对疼痛知觉的影响[J]. 心理科学进展, 2016, 24(8): 1228-1236. |
| [10] | 郑盼盼;吕振勇;Todd Jackson. 疼痛恐惧的形成、泛化与消退[J]. 心理科学进展, 2016, 24(7): 1065-1076. |
| [11] | 杨周;Todd Jackson;陈红;黄承志;苏琳;高婷. 疼痛恐惧相关的注意偏向及其矫正[J]. 心理科学进展, 2016, 24(4): 547-555. |
| [12] | 邓潇斐;罗非;郭建友. 对立的双生子:基于疼痛的安慰剂效应和反安慰剂效应机制[J]. 心理科学进展, 2015, 23(5): 822-835. |
| [13] | 孙泽坤, 王锦琰, 罗非. 疼痛与注意的交互作用:自下而上的捕获效应#br# 和自上而下的调节作用[J]. 心理科学进展, 2015, 23(12): 2096-2106. |
| [14] | 吕振勇;纪晓蕾;黄丽;Todd Jackson;陈红. 疼痛恐惧对疼痛的影响及其认知机制[J]. 心理科学进展, 2013, 21(5): 817-826. |
| [15] | 孟景;沈林;Todd Jackson;陈红. 疼痛对心理的影响及其机制[J]. 心理科学进展, 2011, 19(10): 1493-1501. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||