ISSN 1671-3710
CN 11-4766/R
主办:中国科学院心理研究所
出版:科学出版社
CN 11-4766/R
主办:中国科学院心理研究所
出版:科学出版社
心理科学进展 ›› 2022, Vol. 30 ›› Issue (7): 1561-1573.doi: 10.3724/SP.J.1042.2022.01561 cstr: 32111.14.2022.01561
邓洵, 陈宁, 王单单, 赵欢欢( ), 贺雯()
), 贺雯()
收稿日期:2021-05-24
出版日期:2022-07-15
发布日期:2022-05-17
基金资助:
DENG Xun, CHEN Ning, WANG Dandan, ZHAO Huanhuan(), HE Wen()
Received:2021-05-24
Online:2022-07-15
Published:2022-05-17
摘要:
非自杀性自伤行为(Non-Suicidal Self-Injury, NSSI),简称自伤行为,意为个体在没有明确的自杀意图的情况下,故意、重复地改变或伤害自己的身体组织,是一种不具致死性或致死性较低的、以自身为伤害目标的破坏性行为。本文主要基于近十年的研究文献,从神经生理层面对自伤行为相关脑区、神经递质以及与共病障碍的异同展开述评,并尝试建立一个整合性的自伤行为认知神经机制模型。
关于自伤行为的神经生理机制,综合以往研究发现,自伤患者边缘系统中情绪脑区的异常(如杏仁核的过度激活等)使患者可能产生情绪调节障碍进而导致自伤;控制脑区如前额叶皮层的异常导致其抑制控制能力受损;奖赏脑区如眶额皮层等的过度激活或许会成为自伤复发的维持因素;自伤患者疼痛感知区域如HPA轴的反应水平的减弱使其疼痛敏感性较低并主动追寻疼痛感。除此之外,相关的神经递质和基因的异常也是自伤研究领域关注的重点。比如5-羟色胺转运体其基因连锁多态区的短等位基因会减弱该递质的调节功能,诱使个体出现情绪调节障碍;又比如内源性阿片肽参与了疼痛和情绪调节的过程,且其水平会因个体早期挫折经历和遗传因素而降低,而自伤行为可以促进该递质的释放;同样的,在阿片受体被刺激之后,自伤者体内的多巴胺水平将会升高,个体对自伤行为产生愉悦感。
此外,还将其与自杀、成瘾、进食障碍和抑郁障碍进行了比较。自伤和自杀尝试者在脑电指标上有某些不同的表现,但二者从行为研究和功能成像的角度也呈现出相似性。个体的自伤行为与物质成瘾显著相关,且二者都伴随着抑制控制能力的损伤、阿片类和多巴胺系统异常引发的对某种物质或行为的渴望等。进食障碍患者和自伤行为存在较高的共病率,前者可能就是一种间接的自伤,且二者的脑电和功能成像的指标部分相似。最后,抑郁障碍也是和自伤行为有着较高共病率的一种障碍,部分抑郁障碍患者会通过自伤来调节情绪,且二者有共同的风险因素以及部分重叠的神经机制。研究以上障碍与自伤行为的异同有助于我们从不同角度认识自伤,并多方位实施预警和干预。
在此基础上,本文尝试构建了自伤行为的认知神经机制假设模型,将自伤的认知过程与各阶段起主要作用的神经生理机制相联系。未来的研究可以关注于自伤行为的性别差异、发展特点、干预以及与注意脑区异常的联系等。
中图分类号:
邓洵, 陈宁, 王单单, 赵欢欢, 贺雯. (2022). 自伤行为的神经生理机制及共病障碍比较. 心理科学进展 , 30(7), 1561-1573.
DENG Xun, CHEN Ning, WANG Dandan, ZHAO Huanhuan, HE Wen. (2022). Neural mechanism of NSSI and comparative study with comorbidities. Advances in Psychological Science, 30(7), 1561-1573.
| 作者 | 被试数量 | 年龄 | 研究方法 | 主要结果 |
|---|---|---|---|---|
| 自伤行为 | ||||
| 于丽霞 等, | 自伤组19人 对照组15人 | M = 13.64 | ERP; Go/Nogo任务 | 自伤组Nogo正确反应的N2波幅显著高于对照组, 控制脑区(前额叶)异常。 |
| Dahlgren et al., | 自伤组15人 对照组15人 | 18~31 | fMRI; MSIT任务 | 自伤组控制脑区异常, 扣带回皮层激活更强, 背外侧前额叶激活更弱。 |
| Quevedo et al., | 自伤组50人 抑郁组36人 对照组37人 | M = 14.75 | MRI; 自我认知任务 | 自伤组情绪脑区异常, 杏仁核、楔前叶和后扣带回皮层的活动受社会关系影响。 |
| Schreiner et al., | 自伤组24人 对照组17人 | 13~21 | MRI; 负性情绪面孔匹配范式 | 自伤组情绪脑区异常, 杏仁核与额叶的功能性连接存在缺陷, 与辅助运动区和背侧前扣带回的过度连接。 |
| Hooley et al., | 自伤组15人 对照组15人 | M = 22.03 | fMRI; 呈现不同图片 | 自伤组奖赏脑区异常, 在面对自伤相关图片时, 杏仁核激活更弱, 扣带回皮层和眶额皮层激活更强。 |
| 自杀(自杀意念和自杀尝试) | ||||
| Miller et al., | 自杀意念组14人 对照组35人 | 13~20 | fMR; 情绪调节任务 | 自杀意念组控制脑区异常, 背外侧前额叶激活更强。 |
| Alarcón et al., | 自杀尝试组24人 自杀意念组58人 对照组38人 | 11~18 | MRI; 情绪面孔识别任务 | 自杀尝试组情绪脑区异常, 杏仁核与前扣带回的连接性更强。 |
| Iznak et al., | 自伤组21人 自伤+自杀意念组24人 | M = 18 | ERP; Go/Nogo任务 | 有自杀意念的被试大脑左半球激活更强, 额叶-中央-顶叶区域的脑电相关更强。 |
| 成瘾 | ||||
| Zeng et al., | 成瘾组40人 对照组19人 | 18~45 | fMRI; 呈现不同图片 | 成瘾组在面对与药物使用行为相关的线索更有可能激活中央后回、海马旁回、边缘上回等, 感知运动区域异常。 |
| 郑志灵 等, | 成瘾组20人 对照组20人 | M = 39.84 | ERP; 双选择Oddball范式 | 成瘾组在面对成瘾相关线索时N2波幅更小, 控制和注意脑区有异常。 |
| 进食障碍 | ||||
| Wang et al., | 限制饮食组12人 控制组12人 | M = 20.92 | fMRI | 限制饮食组的奖赏脑区、注意脑区、视觉处理脑区激活更强。 |
| Su et al., | 限制饮食组258人 | M = 20.05 | MRI; VBM | 限制性饮食程度与眶额皮层和左侧脑岛叶的灰质体积正相关, 与扣带回的灰质体积负相关, 控制脑区异常。 |
| Stopyra et al., | 暴食症组27人 神经性贪食症29人 控制组58人 | M1 = 38.39 M2 = 27.45 | fMRI | 患者组背前扣带回和前额叶表现出异常的功能连接, 扣带回和海马过度激活, 控制脑区异常。 |
| Zhou et al., | 限制饮食组40人 | M = 19.93 | ERP; Go/Nogo任务 | 限制性饮食组在对食物相关线索进行抑制时N2波幅更小, 控制脑区异常。 |
| 抑郁障碍 | ||||
| Baeken et al., | 抑郁障碍组12人 对照组12人 | M = 36 | fMRI; 婴儿面孔识别 | 抑郁组在所有条件下前额叶皮层亚属(cg25)激活更强, 控制脑区异常。 |
| 卫芬, | 抑郁障碍组60人 对照组44人 | M=38.2 | ERP | 抑郁组P300波幅更小, 潜伏期更长, 控制脑区异常。 |
| 陈晓鹭 等, | 抑郁患者20人 | M=46.7 | ERP; 情绪Stroop | 被试在不同情绪条件下反应时有差异, ERP的N1、P2、P3波幅有差异, 控制脑区异常。 |
表1 不同障碍脑成像研究文献整理
| 作者 | 被试数量 | 年龄 | 研究方法 | 主要结果 |
|---|---|---|---|---|
| 自伤行为 | ||||
| 于丽霞 等, | 自伤组19人 对照组15人 | M = 13.64 | ERP; Go/Nogo任务 | 自伤组Nogo正确反应的N2波幅显著高于对照组, 控制脑区(前额叶)异常。 |
| Dahlgren et al., | 自伤组15人 对照组15人 | 18~31 | fMRI; MSIT任务 | 自伤组控制脑区异常, 扣带回皮层激活更强, 背外侧前额叶激活更弱。 |
| Quevedo et al., | 自伤组50人 抑郁组36人 对照组37人 | M = 14.75 | MRI; 自我认知任务 | 自伤组情绪脑区异常, 杏仁核、楔前叶和后扣带回皮层的活动受社会关系影响。 |
| Schreiner et al., | 自伤组24人 对照组17人 | 13~21 | MRI; 负性情绪面孔匹配范式 | 自伤组情绪脑区异常, 杏仁核与额叶的功能性连接存在缺陷, 与辅助运动区和背侧前扣带回的过度连接。 |
| Hooley et al., | 自伤组15人 对照组15人 | M = 22.03 | fMRI; 呈现不同图片 | 自伤组奖赏脑区异常, 在面对自伤相关图片时, 杏仁核激活更弱, 扣带回皮层和眶额皮层激活更强。 |
| 自杀(自杀意念和自杀尝试) | ||||
| Miller et al., | 自杀意念组14人 对照组35人 | 13~20 | fMR; 情绪调节任务 | 自杀意念组控制脑区异常, 背外侧前额叶激活更强。 |
| Alarcón et al., | 自杀尝试组24人 自杀意念组58人 对照组38人 | 11~18 | MRI; 情绪面孔识别任务 | 自杀尝试组情绪脑区异常, 杏仁核与前扣带回的连接性更强。 |
| Iznak et al., | 自伤组21人 自伤+自杀意念组24人 | M = 18 | ERP; Go/Nogo任务 | 有自杀意念的被试大脑左半球激活更强, 额叶-中央-顶叶区域的脑电相关更强。 |
| 成瘾 | ||||
| Zeng et al., | 成瘾组40人 对照组19人 | 18~45 | fMRI; 呈现不同图片 | 成瘾组在面对与药物使用行为相关的线索更有可能激活中央后回、海马旁回、边缘上回等, 感知运动区域异常。 |
| 郑志灵 等, | 成瘾组20人 对照组20人 | M = 39.84 | ERP; 双选择Oddball范式 | 成瘾组在面对成瘾相关线索时N2波幅更小, 控制和注意脑区有异常。 |
| 进食障碍 | ||||
| Wang et al., | 限制饮食组12人 控制组12人 | M = 20.92 | fMRI | 限制饮食组的奖赏脑区、注意脑区、视觉处理脑区激活更强。 |
| Su et al., | 限制饮食组258人 | M = 20.05 | MRI; VBM | 限制性饮食程度与眶额皮层和左侧脑岛叶的灰质体积正相关, 与扣带回的灰质体积负相关, 控制脑区异常。 |
| Stopyra et al., | 暴食症组27人 神经性贪食症29人 控制组58人 | M1 = 38.39 M2 = 27.45 | fMRI | 患者组背前扣带回和前额叶表现出异常的功能连接, 扣带回和海马过度激活, 控制脑区异常。 |
| Zhou et al., | 限制饮食组40人 | M = 19.93 | ERP; Go/Nogo任务 | 限制性饮食组在对食物相关线索进行抑制时N2波幅更小, 控制脑区异常。 |
| 抑郁障碍 | ||||
| Baeken et al., | 抑郁障碍组12人 对照组12人 | M = 36 | fMRI; 婴儿面孔识别 | 抑郁组在所有条件下前额叶皮层亚属(cg25)激活更强, 控制脑区异常。 |
| 卫芬, | 抑郁障碍组60人 对照组44人 | M=38.2 | ERP | 抑郁组P300波幅更小, 潜伏期更长, 控制脑区异常。 |
| 陈晓鹭 等, | 抑郁患者20人 | M=46.7 | ERP; 情绪Stroop | 被试在不同情绪条件下反应时有差异, ERP的N1、P2、P3波幅有差异, 控制脑区异常。 |
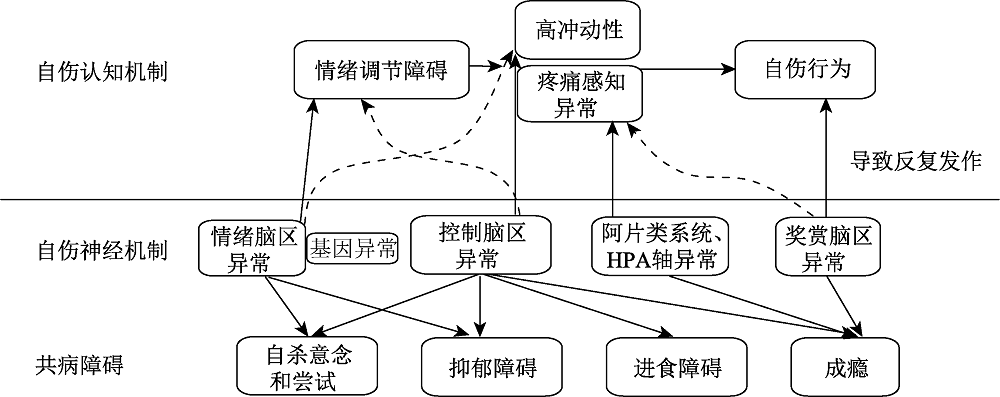
图1 自伤行为的认知神经机制模型
| [1] | 陈世维, 罗显洪, 王霞. (2010). 情感性精神障碍抑郁发作患者个性特征调查. 临床心身疾病杂志, 16(1), 50-51. |
| [2] | 陈晓鹭, 曾金坤, 蒙华庆, 位东涛, 冯正直, 王立菲,... 傅一笑. (2018). 伴自杀意念抑郁症患者事件相关电位的研究. 重庆医科大学学报, 43(2), 176-180. |
| [3] | 国家卫健委. (2020). 新型冠状病毒感染的肺炎疫情紧急心理危机干预指导原则. |
| [4] | 江光荣, 于丽霞, 郑莺, 冯玉, 凌霄. (2011). 自伤行为研究: 现状、问题与建议. 心理科学进展, 19(6), 861-873. |
| [5] | 雷修龙, 许韶君, 刘祥云, 祖萍, 张诗晨, 赵玉秋,... 陶芳标. (2012). 淮北市中学生自伤与自杀行为关系分析. 中国学校卫生, 33(4), 393-395. |
| [6] | 李凡, 舒斯云, 包新民. (2003). 多巴胺受体的结构和功能. 中国神经科学杂志, 19(6), 405-410. |
| [7] | 林云强, 张福娟. (2009). 学生课堂自伤行为的分析及干预策略探讨. 中国特殊教育, (11), 92-96. |
| [8] | 刘珍珍, 汪心婷, 刘贤臣, 王泽颖, 安迪, 贾存显. (2019). 自杀行为暴露与青少年非自杀性自伤关系的纵向研究. 中华流行病学杂志, 40(12), 1573-1577. |
| [9] | 鲁婷, 江光荣, 于丽霞, 应梦婷, 韦辉, 林秀彬. (2015). 自伤者对不同情绪调节方式的注意偏向. 中国临床心理学杂志, 23(3), 431-434, 493. |
| [10] | 美国精神医学学会, 张道龙. (2016). 精神障碍诊断与统计手册. 北京大学出版社. |
| [11] | 潘珍, 毛绍菊, 唐寒梅, 傅燕艳, 孙玮璇, 廖志林,... 朱金云. (2016). 中国大学生非自杀性自伤检出率的Meta分析. 中国学校卫生, 37(6), 878-881. |
| [12] | 庞卢伟, 赵幸福. (2011). 抑郁症与多巴胺受体及转运体基因关联研究进展. 新乡医学院学报, 28(5), 636-639. |
| [13] | 苏普玉, 郝加虎, 黄朝辉, 陶芳标. (2010). 2713名大学生自伤行为及其与自杀心理行为的关联研究. 中华流行病学杂志, 31(11), 1267-1271. |
| [14] | 王路, 刘君, 屈燕花, 邹海欧. (2020). 心境障碍患者非自杀性自伤行为现状及影响因素研究. 精神医学杂志, 33(2), 134-139. |
| [15] | 王曼, 陶嵘, 胡姝婧, 朱旭. (2011). 注意偏向训练:起源、 效果与机制. 心理科学进展, 19(3), 390-397. |
| [16] | 王泉泉, 熊昱可, 刘霞. (2019). 基因-脑-行为视角下的自伤行为产生机制. 心理发展与教育, 35(4), 495-503. |
| [17] | 卫芬. (2013). 抑郁症患者脑电图与事件相关电位结果分析. 现代诊断与治疗, (15), 3555-3556. |
| [18] | 吴燕, 王建峰, 温馨, 景璐石, 杨奇伟. (2017). 情绪智力和性别对情绪调节过程的影响. 中华行为医学与脑科学杂志, 26(11), 1030-1035. |
| [19] | 肖晶, 朱雪玲, 罗英姿, 张小崔, 何晓燕, 王湘, 姚树桥. (2011). 抑郁症的脑结构异常—结构性磁共振成像研究进展. 中国临床心理学杂志, (5), 589-590+608. |
| [20] | 谢祥龙, 刘珍, 陈艳, 劳颖欣, 江雅琴. (2016). 大学生强化敏感性对网络游戏成瘾的影响:网络游戏动机的中介效应. 中国健康心理学杂志, 24(5), 771-775. |
| [21] | 辛秀红, 姚树桥. (2016). 青少年直接自伤行为的发生率及与生活事件的关系. 中国临床心理学杂志, 24(1), 124-128. |
| [22] | 星一, 乔毅娟, 段佳丽, 白承续. (2015). 北京市中学生自我伤害行为现状及与自杀相关行为关系的研究. 中华流行病学杂志, 36(9), 921-924. |
| [23] | 薛艳芝, 鲁显福, 胡啸玲, 王佑陵. (2019). 疼痛性别差异的表观遗传学研究进展. 中国疼痛医学杂志, 25(12), 928-932. |
| [24] | 颜赟慈. (2015). 自伤行为中疼痛和见血的情绪调节作用 (硕士学位论文). 华中师范大学, 武汉. |
| [25] | 杨军, 谢宇平, 周丽雅, 马薇, 惠培林, 范杰, 陈文娟. (2020). 5-羟色胺转运体基因多态性与睡眠障碍的相关性研究进展. 精神医学杂志, 33(1), 78-80. |
| [26] | 应梦婷, 江光荣, 于丽霞, 鲁婷. (2016). 大学生自伤行为的强化敏感性基础. 心理学报, 48(3), 258-270. |
| [27] | 于丽霞, 凌霄, 江光荣. (2013). 自伤青少年的冲动性. 心理学报, 45(3), 320-335. |
| [28] | 张永超. (2014). 5-羟色胺受体与抑郁症相关性的研究进展. 医学综述, 20(5), 772-775. |
| [29] | 郑志灵, 王鹏飞, 苏得权, 郭伟杰, 孙楠, 麻彦坤, 曾红. (2020). 不同相关线索下海洛因成瘾者的反应差异及反应抑制特征: 来自ERP的证据. 心理学报, 52(3), 371-328. |
| [30] | Ahn, J., Lee, J., & Jung, Y. (2021). Identifying predictors of non-suicidal self-injuries in individuals with eating disorders. Yonsel Medical Journal, 62(2), 159-163. |
| [31] | Alarcón, G., Sauder, M., Teoh, J. Y., Forbes, E. E., & Quevedo, K. (2019). Amygdala functional connectivity during self-face processing in depressed adolescents with recent suicide attempt. Journal of the American Academy of Child and Adolescent Psychiatry, 58(2), 221-231. |
| [32] | Allen, K. J. D., Sammon, M. M., Fox, K. R., & Stewart, J. G. (2020). Emotional response inhibition: A shared neurocognitive deficit in eating disorder symptoms and non-suicidal self-injury. Brain Sciences, 10(2), Article 104. https://doi.org/10.20944/preprints201912.0193.v1 |
| [33] |
Anderson, N. L., Smith, K. E., Mason, T. B., & Crowther, J. H. (2018). Testing an integrative model of affect regulation and avoidance in non-suicidal self-injury and disordered eating. Archives of Suicide Research, 22(2), 295-310.
doi: 10.1080/13811118.2017.1340854 URL |
| [34] |
Auerbach, R. P., Pagliaccio, D., Allison, G. O., Alqueza, K. L., & Alonso, M. F. (2021). Neural correlates associated with suicide and nonsuicidal self-injury in youth. Biological Psychiatry, 89(2), 119-133.
doi: 10.1016/j.biopsych.2020.06.002 pmid: 32782140 |
| [35] |
Baeken, C., van Schuerbeek, P., de Raedt, R., Ramsey, N. F., Bossuyt, A., de Mey, J., … Luypaert, R. (2010). Reduced left subgenual anterior cingulate cortical activity during withdrawal-related emotions in melancholic depressed female patients. Journal of Affective Disorders, 127(1-3), 326-331.
doi: 10.1016/j.jad.2010.02.117 URL |
| [36] |
Balázs, J., Győri, D., Horváth, L. O., Mészáros, G., & Szentiványi, D. (2018). Attention-deficit hyperactivity disorder and nonsuicidal self-injury in a clinical sample of adolescents: The role of comorbidities and gender. BMC Psychiatry, 18(1), 34.
doi: 10.1186/s12888-018-1620-3 pmid: 29409473 |
| [37] |
Ballard, E., Bosk, A., & Pao, M. (2010). Invited commentary: Understanding brain mechanisms of pain processing in adolescents' non-suicidal self-injury. Journal of Youth and Adolescence, 39(4), 327-334
doi: 10.1007/s10964-009-9457-1 URL |
| [38] |
Bresin, K., & Gordon, K. H. (2013). Endogenous opioids and nonsuicidal self-injury: A mechanism of affect regulation. Neuroscience and Biobehavioral Reviews, 37(3), 374-383.
doi: 10.1016/j.neubiorev.2013.01.020 URL |
| [39] |
Bunderla, T., & Kumperščak, H. G. (2015). Altered pain perception in self-injurious behavior and the association of psychological elements with pain perception measures: A systematic review. Psychiatria Danubina, 27(4), 346-354.
pmid: 26609646 |
| [40] | Buser, T. J., & Buser, J. K. (2013). Conceptualizing nonsuicidal self-injury as a process addiction: Review of research and implications for counselor training and practice. Journal of Addictions & Offender Counseling, 34(1), 16-29. |
| [41] | Cassels, M., Neufeld, S., van Harmelen, A., Goodyer, I., & Wilkinson, P. (2020). Prospective pathways from impulsivity to non-suicidal self-injury among youth. Archives of Suicide Research, 24, 1-14. |
| [42] | Chan, M. K. Y., Bhatti, H., Meader, N., Stockton, S., Evans, J., O'Connor, R. C.,... Kendall, T. (2016). Predicting suicide following self-harm: Systematic review of risk factors and risk scales. British Journal of Psychiatry, 209(4), 279-285. |
| [43] |
Claes, L., Buelens, T., Depestele, L., Dierckx, E., Schoevaerts, K., & Luyckx, K. (2021). Obsessive-compulsive symptoms in female patients with an eating disorder with or without impulsive non-suicidal self-injury. European Eating Disorders Review, 29(4), 663-669.
doi: 10.1002/erv.2836 URL |
| [44] |
Claes, L., Fagundo, A. B., Jiménez-Murcia, S., Agüera, Z., Giner-Bartolome, C., Granero, R.,... Fernandez-Aranda, F. (2015). Is non-suicidal self-injury related to impulsivity in anorexia nervosa? Results from self-report and performance-based tasks. European Eating Disorders Review, 23(1), 28-33.
doi: 10.1002/erv.2329 URL |
| [45] |
Claes, L., Jiménez-Murcia, S., Agüera, Z., Castro, R., Sánchez, I., Menchón, J. M.,... Fernández-Aranda, F. (2012). Male eating disorder patients with and without non-suicidal self-injury: A comparison of psychopathological and personality features. European Eating Disorders Review, 20(4), 335-338.
doi: 10.1002/erv.1161 URL |
| [46] | Cullen, K. R., Schreiner, M. W., Klimes-Dougan, B., Eberly, L. E., LaRiviere, L. L., Lim, K. O.,... Mueller, B. A. (2020). Neural correlates of clinical improvement in response to N-acetylcysteine in adolescents with non-suicidal self-injury. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 99, Article 109778. https://doi.org/10.1016/j.pnpbp.2019.109778 |
| [47] |
Dahlgren, M. K., Hooley, J. M., Best, S. G., Sagar, K. A., Gonenc, A., & Gruber, S. A. (2018). Prefrontal cortex activation during cognitive interference in nonsuicidal self-injury. Psychiatry Research: Neuroimaging, 277, 28-38.
doi: 10.1016/j.pscychresns.2018.04.006 URL |
| [48] |
Davis, S., & Lewis, C. A. (2019). Addiction to self-harm? The case of online postings on self-harm message boards. International Journal of Mental Health and Addiction, 17(4), 1020-1035.
doi: 10.1007/s11469-018-9975-8 URL |
| [49] | Drevets, W. C. (2010). Neuroimaging abnormalities in the amygdala in mood disorders. Annals of the New York Academy of Sciences, 985(1), 420-444. |
| [50] |
Escelsior, A., Murri, M. B., Corsini, G. P., Serafini, G., Aguglia, A., Zampogna, D., … Amore, M. (2021). Cannabinoid use and self-injurious behaviours: A systematic review and meta-analysis. Journal of Affective Disorders, 278, 85-98.
doi: 10.1016/j.jad.2020.09.020 pmid: 32956965 |
| [51] | Esposito, C., Spirito, A., Boergers, J., & Donaldson, D. (2003). Affective, behavioral, and cognitive functioning in adolescents with multiple suicide attempts. Suicide & Life-threatening Behavior, 33(4), 389-399. |
| [52] |
Faye, P. (1995). Addictive characteristics of the behavior of self-mutilation. Journal of Psychosocial Nursing and Mental Health Services, 33(6), 36-39.
doi: 10.3928/0279-3695-19950601-08 pmid: 7666387 |
| [53] | Few, L. R., Grant, J. D., Nelson, E. C., Trull, T. J., Grucza, R. A., Bucholz, K. K.,... Agrawal, A. (2016). Cannabis involvement and nonsuicidal self-injury: A discordant twin approach. Journal of Studies on Alcohol & Drugs, 77(6), 873-880. |
| [54] | Gatta, M., Dal Santo, F., Rago, A., Spoto, A., & Battistella, P. A. (2016). Alexithymia, impulsiveness, and psychopathology in nonsuicidal self-injured adolescents. Neuropsychiatry Disorder Treatment, 12, 2307-2317. |
| [55] |
Glenn, C. R., & Klonsky, E. D. (2010). A multimethod analysis of impulsivity in nonsuicidal self-injury. Personal Disorder, 1(1), 67-75.
doi: 10.1037/a0017427 URL |
| [56] |
Gratz, K. L. (2001). Measurement of deliberate self-harm: Preliminary data on the deliberate self-harm inventory. Journal of Psychopathology and Behavioral Assessment, 23(4), 253-263.
doi: 10.1023/A:1012779403943 URL |
| [57] | Hay, P. (2020). Current approach to eating disorders: A clinical update. Internal Medicine Journal, 50(1), 24-29. |
| [58] |
Hayes, S. C., Masuda, A., Bissett, R., Luoma, J., & Guerrero, L. F. (2005). DBT, FAP, and ACT: How empirically oriented are the new behavior therapy technologies? Behavior Therapy, 35(1), 35-54.
doi: 10.1016/S0005-7894(04)80003-0 URL |
| [59] | Hilario, B. F., Roberto, F. F., Laura, C., Lourdes, F., Rosa, P. B., & Jose, D. L. (2016). The addictive model of self-harming (non-suicidal and suicidal) behavior. Frontiers in Psychiatry, 7, Article 8. https://doi.org/10.3389/fpsyt.2016.00008 |
| [60] | Hooley, J. M., Dahlgren, M. K., Best, S. G., Gonenc, A., & Gruber, S. A. (2020). Decreased amygdalar activation to NSSI-stimuli in people who engage in NSSI: A neuroimaging pilot study. Front Psychiatry, 11, Article 238. https://doi.org/10.3389/fpsyt.2020.00238 |
| [61] |
Iznak, A. F., Iznak, E. V., Damyanovich, E. V., & Oleichik, I. V. (2021). Differences of EEG frequency and spatial parameters in depressive female adolescents with suicidal attempts and non-suicidal self-injuries. Clinical EEG and Neuroscience, 52(6), 406-413.
doi: 10.1177/1550059421991685 URL |
| [62] |
Janis, I. B., & Nock, M. K. (2009). Are self-injurers impulsive? Results from two behavioral laboratory studies. Psychiatry Research, 169(3), 261-267.
doi: 10.1016/j.psychres.2008.06.041 URL |
| [63] |
Karwautz, A., Resch, F., Wöber-Bingöl, C., & Schuch, B.. (1996). Self-mutilation in adolescence as addictive behaviour. Wiener Klinische Wochenschrift, 108(3), 82-84.
pmid: 8839194 |
| [64] |
Kim, K. L., Galvan, T., Puzia, M. E., Cushman, G. K., Seymour, K. E., Vanmali, R.,... Dickstein, D. P. (2015). Psychiatric and self-injury profiles of adolescent suicide attempters versus adolescents engaged in nonsuicidal self-injury. Suicide Life Threat Behavior, 45(1), 37-50.
doi: 10.1111/sltb.12110 URL |
| [65] |
Koenig, J., Rinnewitz, L., Warth, M., Hillecke, T. K., Brunner, R., Resch, F., & Kaess, M. (2017). Psychobiological response to pain in female adolescents with nonsuicidal self-injury. Journal of Psychiatry Neuroscience, 42(3), 189-199.
doi: 10.1503/jpn.160074 URL |
| [66] |
Krantz, L. H., McMain, S., & Kuo, J. R. (2018). The unique contribution of acceptance without judgment in predicting nonsuicidal self-injury after 20-weeks of dialectical behaviour therapy group skills training. Behaviour Research and Therapy, 104, 44-50.
doi: 10.1016/j.brat.2018.02.006 URL |
| [67] |
Kraus, L., Schmid, M., & In-Albon, T. (2020). Anti-Suicide function of nonsuicidal self-injury in female inpatient adolescents. Frontiers in Psychiatry, 11, 490.
doi: 10.3389/fpsyt.2020.00490 URL |
| [68] |
Maciejewski, D. F., Renteria, M. E., Abdellaoui, A., Medland, S. E., Few, L. R., Gordon, S. D.,... Verweij, K. J. (2017). The association of genetic predisposition to depressive symptoms with non-suicidal and suicidal self-injuries. Behavior Genetics, 47(1), 3-10.
doi: 10.1007/s10519-016-9809-z pmid: 27590903 |
| [69] |
Miller, A. B., Mclaughlin, K. A., Busso, D. S., Brueck, S., Peverill, M., & Sheridan, M. A. (2018). Neural correlates of emotion regulation and adolescent suicidal ideation. Biological Psychiatry: Cognitive Neuroscience and Neuroimaging, 3(2), 125-132.
doi: 10.1016/j.bpsc.2017.08.008 URL |
| [70] |
Miller, E. K., & Cohen, J. D. (2001). An integrative theory of prefrontal cortex function. Annual Review of Neuroscience, 24(1), 167-202.
doi: 10.1146/annurev.neuro.24.1.167 URL |
| [71] |
Muehlenkamp, J. J., Suzuki, T., Brausch, A. M., & Peyerl, N. (2019). Behavioral functions underlying NSSI and eating disorder behaviors. Journal of Clinical Psychology, 75(7), 1219-1232.
doi: 10.1002/jclp.22745 pmid: 30672588 |
| [72] |
Muehlmann, A. M., Wolfman, S. L., & Devine, D. P. (2018). The role of neurotensin in vulnerability for self-injurious behaviour: Studies in a rodent model. Journal of Intellectual Disability Research, 62(12), 997-1007.
doi: 10.1111/jir.12519 pmid: 30033601 |
| [73] |
Nixon, M. K., Cloutier, P. F., & Aggarwal, S. (2002). Affect regulation and addictive aspects of repetitive Self-Injury in hospitalized adolescents. Journal of the American Academy of Child & Adolescent Psychiatry, 41(11), 1333-1341.
doi: 10.1097/00004583-200211000-00015 URL |
| [74] |
Nock, M. K. (2009). Why do People hurt themselves? New insights into the nature and functions of Self-Injury. Current Directions in Psychological Science, 18(2), 78-83.
doi: 10.1111/j.1467-8721.2009.01613.x URL |
| [75] |
Quevedo, K., Martin, J., Scott, H., Smyda, G., & Pfeifer, J. H. (2016). The neurobiology of self-knowledge in depressed and self-injurious youth. Psychiatry Research: Neuroimaging, 254, 145-155.
doi: 10.1016/j.pscychresns.2016.06.015 URL |
| [76] |
Ran, H., Fang, D., Donald, A. R., Wang, R., Che, Y., He, X.,... Xiao, Y. (2021). Impulsivity mediates the association between parenting styles and self-harm in Chinese adolescents. BMC Public Health, 21(1), 332.
doi: 10.1186/s12889-021-10386-8 URL |
| [77] |
Reitz, S., Kluetsch, R., Niedtfeld, I., Knorz, T., Lis, S., Paret, C.,... Schmahl, C. (2015). Incision and stress regulation in borderline personality disorder: Neurobiological mechanisms of self-injurious behaviour. British Journal of Psychiatry, 207(2), 165-172.
doi: 10.1192/bjp.bp.114.153379 URL |
| [78] |
Rinnewitz, L., Koenig, J., Parzer, P., Brunner, R., Resch, F., & Kaess, M. (2018). Childhood adversity and psychophysiological reactivity to pain in adolescent nonsuicidal self-injury. Psychopathology, 51(5), 346-352.
doi: 10.1159/000491702 pmid: 30157488 |
| [79] | Sahlin, H., Bjureberg, J., Gratz, K. L., Tull, M. T., Hedman, E., Bjärehed, J.,... Hellner, C. (2017). Emotion regulation group therapy for deliberate self-harm: A multi-site evaluation in routine care using an uncontrolled open trial design. BMJ Open, 7(10), Article e016220. https://doi.org/10.1136/bmjopen-2017-016220. |
| [80] | Salinas-Hernández, X. I., & Duvarci, S. (2021). Dopamine in fear extinction. Frontiers in Synaptic Neuroscience, 13, Article 635879. https://doi.org/10.3389/fnsyn.2021.635879. |
| [81] |
Santamarina-Perez, P., Romero, S., Mendez, I., Leslie, S. M., Packer, M. M., Sugranyes, G.,... Singh, M. K. (2019). Fronto-limbic connectivity as a predictor of improvement in nonsuicidal self-injury in adolescents following psychotherapy. Journal of Child and Adolescent Psychopharmacology, 29(6), 456-465.
doi: 10.1089/cap.2018.0152 pmid: 31225733 |
| [82] | Schloss, N., Shabes, P., Kuniss, S., Willis, F., Treede, R. D., Schmahl, C.,... Baumgärtner, U. (2019). Differential perception of sharp pain in patients with borderline personality disorder. Europe Journal of Pain, 23(8), 1448-1463. |
| [83] |
Schreiner, M. W., Klimes-Dougan, B., Mueller, B. A., Eberly, L. E., Reigstad, K. M., Carstedt, P. A.,... Cullen, K. R. (2017). Multi-modal neuroimaging of adolescents with non-suicidal self-injury: Amygdala functional connectivity. Journal of Affective Disorders, 221, 47-55.
doi: S0165-0327(16)31545-2 pmid: 28628767 |
| [84] |
Sinyor, M., Williams, M., Mitchell, R., Zaheer, R., Bryan, C. J., Schaffer, A.,... Tien, H. (2020). Cognitive behavioral therapy for suicide prevention in youth admitted to hospital following an episode of self-harm: A pilot randomized controlled trial. Journal of Affective Disorder, 266, 686-694.
doi: 10.1016/j.jad.2020.01.178 URL |
| [85] |
Stanley, B., Sher, L., Wilson, S., Ekman, R., Huang, Y. Y.,... Mann, J. J. (2010). Non-suicidal self-injurious behavior, endogenous opioids and monoamine neurotransmitters. Journal of Affective Disorder, 124(1-2), 134-140.
doi: 10.1016/j.jad.2009.10.028 URL |
| [86] | Stopyra, M. A., Simon, J. J., Skunde, M., Walther, S., Bendszus, M., Herzog, W.,... Friederich, H. C. (2019). Altered functional connectivity in binge eating disorder and bulimia nervosa: A resting‐state fMRI study. Brain and Behavior, 9(2), Article e01207. https://doi.org/10.1002/brb3.1207 |
| [87] |
Störkel, L. M., Karabatsiakis, A., Hepp, J., Kolassa, I. T., Schmahl, C., & Niedtfeld, I. (2021). Salivary beta-endorphin in nonsuicidal self-injury: An ambulatory assessment study. Neuropsychopharmacology, 46, 1357-1363.
doi: 10.1038/s41386-020-00914-2 pmid: 33398083 |
| [88] | Su, Y., Jackson, T., Wei, D., Qiu, J., & Chen, H. (2017). Regional gray matter volume is associated with restrained eating in healthy Chinese young adults: Evidence from voxel-based morphometry. Frontiers in Psychology, 8, Article 443. https://doi.org/10.3389/fpsyg.2017.00443. |
| [89] |
Turner, B. J., Yiu, A., Layden, B. K., Claes, L., Zaitsoff, S., & Chapman, A. L. (2015). Temporal associations between disordered eating and nonsuicidal self-injury: Examining symptom overlap over 1 year. Behavior Therapy, 46(1), 125-138.
doi: 10.1016/j.beth.2014.09.002 URL |
| [90] |
Vega, D., Ripollés, P., Soto, À., Torrubia, R., Ribas, J., Monreal, J. A.,... Marco-Pallarés, J. (2018). Orbitofrontal overactivation in reward processing in borderline personality disorder: The role of non-suicidal self-injury. Brain Imaging Behavior, 12(1), 217-228.
doi: 10.1007/s11682-017-9687-x URL |
| [91] |
Victor, S. E., Glenn, C. R., & Klonsky, E. D. (2012). Is non-suicidal self-injury an "addiction"? A comparison of craving in substance use and non-suicidal self-injury. Psychiatry Research, 197(1-2), 73-77.
doi: 10.1016/j.psychres.2012.02.013 URL |
| [92] |
Victor, S. E., Muehlenkamp, J. J., Hayes, N. A., Lengel, G. J., Styer, D. M., & Washburn, J. J. (2018). Characterizing gender differences in nonsuicidal self-injury: Evidence from a large clinical sample of adolescents and adults. Comprehensive Psychiatry, 82, 53-60.
doi: S0010-440X(18)30015-4 pmid: 29407359 |
| [93] |
Volkow, N. D., Koob, G. F., & Mclellan, A. T. (2016). Neurobiologic advances from the brain disease model of addiction. New England Journal of Medicine, 374(4), 363-371.
doi: 10.1056/NEJMra1511480 URL |
| [94] |
Wang, Q., & Liu, X. (2019). Peer victimization, depressive symptoms and non-suicidal self-injury behavior in Chinese migrant children: The roles of gender and stressful life events. Psychology Research and Behavior Management, 12, 661-673.
doi: 10.2147/PRBM.S215246 URL |
| [95] |
Wang, Y., Dong, D., Todd, J., Du, J., Yang, Z., Lu, H., & Chen, H. (2016). Neural correlates of restrained eaters' high susceptibility to food cues: An fMRI study. Neuroscience Letters, 631, 56-62.
doi: S0304-3940(16)30588-2 pmid: 27524674 |
| [96] |
Warne, N., Heron, J., Mars, B., Moran, P., Stewart, A., Munafo, M.,... Bould, H. (2021). Comorbidity of self-harm and disordered eating in young people: Evidence from a UK population-based cohort. Journal of Affective Disorder, 282, 386-390.
doi: 10.1016/j.jad.2020.12.053 URL |
| [97] |
Worley, J. (2017). The role of pleasure neurobiology and dopamine in mental health disorders. Journal of Psychosocial Nursing and Mental Health Services, 55(9), 17-21.
doi: 10.3928/02793695-20170818-09 pmid: 28850647 |
| [98] |
Yang, X., & Xin, M. (2018). “Boy Crisis” or “Girl Risk”? The gender difference in nonsuicidal self-injurious behavior among middle-school students in China and its relationship to gender role conflict and violent experiences. American Journal of Men's Health, 12(5), 1275-1285.
doi: 10.1177/1557988318763522 URL |
| [99] | Ye, D. H., Hong, H. J., Yook, K. H., Choi, H. I., Lee, J. E., Jun, J. Y., … Song, J. E. (2012). Psychosocial factors that influence on non-suicidal self-injury in depressed adolescents. Journal of Korean Social Depress Bipolar Disorder, 10(2), 85-90. |
| [100] |
You, J, N., Zheng, C. H., Lin, M. P., & Leung, F. (2016). Peer group impulsivity moderated the individual-level relationship between depressive symptoms and adolescent nonsuicidal self-injury. Journal of Adolescence, 47, 90-99.
doi: 10.1016/j.adolescence.2015.12.008 URL |
| [101] | Zeng, H., Su, D., Wang, P., Wang, M., Vollstädt-Klein, S., Chen, Q., Ye, H. (2018). The action representation elicited by different types of drug-related cues in heroin-abstinent individuals. Frontiers in Behavioral Neuroscience, 12, Article 123. https://doi.org/10.3389/fnbeh.2018.00123 |
| [102] |
Zhou, Y., Liu, Y., Du, J., & Chen, H. (2018). Effects of food exposure on food-related inhibitory control in restrained eaters: An ERP study. Neuroscience Letters, 672, 130-135.
doi: 10.1016/j.neulet.2018.02.048 URL |
| [1] | 高白雪, 谢云龙, 罗俊龙, 贺雯. 机器学习在提高非自杀性自伤预测力中的应用:一项系统综述[J]. 心理科学进展, 2025, 33(3): 506-519. |
| [2] | 蒋家丽, 李立言, 李子颖, 雷秀雅, 孟泽龙. 青少年非自杀性自伤行为持续和停止的预测性因素[J]. 心理科学进展, 2022, 30(7): 1536-1545. |
| [3] | 杨廙, 李东, 崔倩, 蒋重清. 触觉的情绪功能及其神经生理机制[J]. 心理科学进展, 2022, 30(2): 324-332. |
| [4] | 张霞, 雷怡, 王福顺. 催产素、孕激素和雌激素对厌恶的影响及其神经生理机制[J]. 心理科学进展, 2022, 30(1): 85-97. |
| [5] | 马原啸, 陈旭. 非安全依恋可塑性的神经机制[J]. 心理科学进展, 2019, 27(12): 1967-1979. |
| [6] | 杨伟星;张明亮;李红霞;杨雅琳;司继伟. 人类基本数学能力的进化证据[J]. 心理科学进展, 2017, 25(5): 810-824. |
| [7] | 郭丰波;张振;原胜;敬一鸣;王益文. 自恋型人格的理论模型与神经生理机制[J]. 心理科学进展, 2016, 24(8): 1246-1256. |
| [8] | 郝亚楠;宋勃东;王岩;张钦;郎越. 气质性乐观的正性偏向及其神经生理研究证据[J]. 心理科学进展, 2016, 24(6): 946-957. |
| [9] | 钟歆;陈旭. 不同依恋风格者对情绪面孔的加工[J]. 心理科学进展, 2013, 21(12): 2154-2163. |
| [10] | 江光荣;于丽霞;郑莺;冯玉;凌霄. 自伤行为研究:现状、问题与建议[J]. 心理科学进展, 2011, 19(6): 861-873. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||