ISSN 0439-755X
CN 11-1911/B
CN 11-1911/B
Acta Psychologica Sinica ›› 2022, Vol. 54 ›› Issue (12): 1503-1516.doi: 10.3724/SP.J.1041.2022.01503
• Reports of Empirical Studies • Previous Articles Next Articles
WANG Wenchao1, YUAN Hao2,1, WU Xinchun1( )
)
Published:2022-12-20
Online:2022-09-23
Contact:
WU Xinchun
E-mail:xcwu@bnu.edu.cn
WANG Wenchao, YUAN Hao, WU Xinchun. (2022). Co-morbidity patterns of posttraumatic stress disorder and depressive symptoms: A network analysis of post-earthquake primary and secondary school students. Acta Psychologica Sinica, 54(12), 1503-1516.

Figure 1. The standardized centrality index of each node in the network.
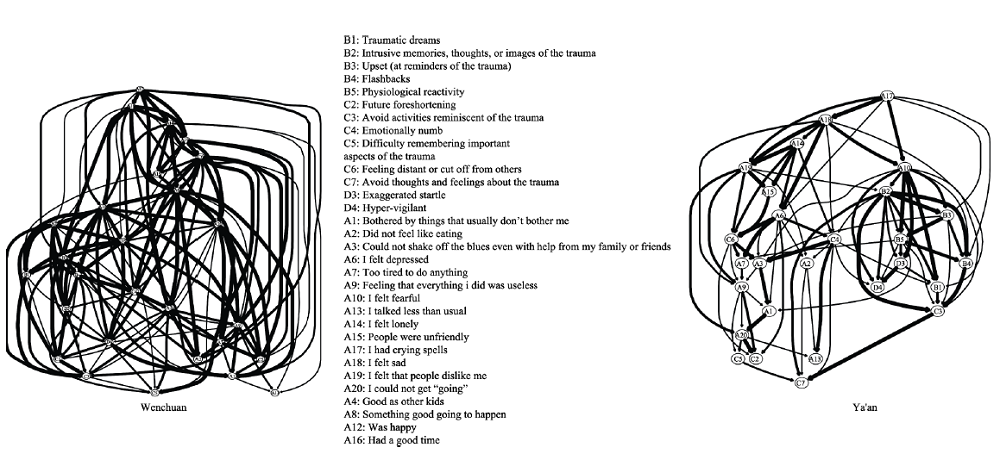
Figure 2. DAG of Wenchuan and Ya 'an samples (excluding overlapping symptoms).
| B2 | B3 | B4 | B5 | C1 | C2 | C3 | C4 | C5 | C6 | C7 | D1 | D2 | D3 | D4 | D5 | A1 | A2 | A3 | A5 | A6 | A7 | A9 | A10 | A11 | A13 | A14 | A15 | A17 | A18 | A19 | A20 | A4 | A8 | A12 | A16 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B1 | 0.094 | 0.036 | 0.010 | 0.035 | 0.000 | -0.009 | 0.050 | 0.000 | 0.002 | -0.035 | 0.078 | 0.000 | 0.175 | 0.075 | 0.001 | 0.034 | 0.000 | 0.022 | 0.007 | -0.003 | 0.002 | 0.000 | 0.000 | 0.137 | 0.054 | 0.000 | 0.000 | 0.025 | 0.000 | 0.000 | 0.005 | -0.018 | 0.000 | 0.016 | 0.004 | 0.000 |
| B2 | 0.172 | 0.171 | 0.057 | 0.000 | -0.009 | 0.128 | 0.031 | 0.000 | -0.011 | 0.076 | 0.032 | 0.000 | 0.068 | 0.061 | 0.011 | 0.000 | 0.007 | 0.000 | -0.010 | 0.000 | 0.000 | 0.000 | 0.070 | 0.026 | 0.010 | 0.000 | -0.009 | 0.008 | 0.020 | -0.005 | 0.000 | 0.048 | 0.000 | 0.000 | 0.005 | |
| B3 | 0.101 | 0.173 | 0.018 | 0.000 | 0.089 | 0.038 | -0.006 | -0.055 | 0.053 | 0.000 | 0.010 | 0.058 | 0.000 | 0.002 | 0.051 | 0.043 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.052 | 0.000 | 0.020 | -0.013 | -0.018 | 0.056 | 0.073 | -0.009 | 0.000 | 0.017 | -0.003 | 0.000 | 0.016 | ||
| B4 | 0.157 | 0.000 | 0.005 | 0.082 | 0.069 | 0.039 | 0.000 | 0.011 | 0.000 | 0.000 | 0.074 | 0.045 | 0.000 | 0.042 | 0.015 | 0.000 | 0.000 | 0.000 | 0.000 | 0.022 | 0.064 | 0.013 | 0.000 | -0.011 | 0.014 | 0.007 | 0.000 | 0.000 | 0.006 | 0.015 | 0.000 | -0.021 | 0.000 | |||
| B5 | 0.000 | 0.000 | 0.095 | 0.042 | 0.025 | -0.001 | 0.059 | 0.010 | 0.015 | 0.006 | 0.052 | 0.000 | 0.015 | 0.006 | 0.018 | 0.000 | 0.009 | 0.012 | 0.000 | 0.103 | 0.022 | 0.018 | -0.002 | 0.000 | 0.000 | 0.000 | -0.005 | 0.008 | -0.023 | 0.026 | 0.000 | -0.004 | ||||
| C1 | 0.050 | 0.069 | 0.029 | 0.015 | 0.061 | 0.049 | 0.073 | 0.066 | 0.013 | 0.006 | 0.024 | 0.047 | 0.010 | 0.006 | 0.024 | 0.047 | 0.016 | 0.040 | 0.000 | 0.000 | 0.036 | 0.000 | 0.000 | 0.000 | -0.009 | 0.000 | 0.041 | 0.000 | 0.000 | -0.012 | 0.000 | |||||
| C2 | 0.001 | 0.001 | 0.011 | 0.109 | -0.011 | 0.083 | 0.032 | 0.046 | 0.021 | 0.017 | 0.050 | 0.000 | 0.000 | 0.033 | 0.000 | 0.063 | 0.067 | 0.000 | 0.000 | 0.000 | 0.031 | 0.000 | -0.012 | 0.000 | 0.058 | 0.080 | 0.000 | -0.004 | -0.014 | -0.025 | ||||||
| C3 | 0.015 | 0.008 | 0.000 | 0.143 | 0.000 | 0.020 | 0.017 | 0.048 | -0.019 | 0.000 | -0.003 | 0.017 | -0.026 | 0.000 | 0.000 | 0.000 | 0.018 | 0.003 | 0.000 | 0.000 | 0.000 | 0.003 | 0.010 | 0.000 | 0.000 | -0.005 | 0.007 | 0.000 | 0.000 | |||||||
| C4 | 0.023 | 0.062 | 0.003 | 0.061 | 0.070 | 0.022 | 0.040 | 0.051 | 0.003 | 0.023 | 0.128 | 0.000 | 0.057 | 0.045 | 0.014 | 0.011 | 0.010 | 0.026 | 0.027 | 0.009 | 0.019 | 0.053 | 0.000 | 0.028 | 0.000 | 0.000 | 0.000 | -0.011 | ||||||||
| C5 | 0.069 | 0.055 | 0.002 | 0.000 | -0.016 | 0.037 | 0.036 | 0.010 | 0.010 | 0.048 | 0.000 | 0.000 | 0.024 | 0.000 | 0.039 | 0.005 | 0.014 | 0.000 | 0.031 | -0.004 | -0.036 | 0.000 | 0.056 | 0.000 | 0.009 | 0.015 | 0.007 | |||||||||
| C6 | 0.000 | 0.021 | 0.009 | 0.023 | 0.024 | 0.150 | 0.003 | 0.000 | 0.058 | 0.012 | 0.045 | 0.045 | 0.042 | -0.034 | 0.018 | 0.037 | 0.141 | 0.066 | 0.000 | 0.001 | 0.118 | 0.065 | -0.001 | 0.000 | -0.009 | 0.000 | ||||||||||
| C7 | 0.019 | 0.000 | 0.000 | 0.048 | 0.000 | 0.000 | 0.041 | 0.055 | -0.005 | -0.004 | 0.000 | 0.046 | 0.003 | 0.000 | 0.006 | -0.007 | 0.000 | 0.000 | -0.002 | 0.000 | 0.020 | 0.000 | 0.020 | 0.000 | 0.032 | |||||||||||
| D1 | 0.109 | 0.013 | 0.000 | 0.043 | 0.010 | 0.000 | 0.000 | 0.295 | 0.029 | 0.003 | 0.055 | 0.010 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.039 | 0.000 | 0.000 | -0.033 | 0.000 | ||||||||||||
| D2 | 0.047 | 0.047 | 0.004 | 0.000 | 0.042 | 0.000 | 0.051 | 0.000 | 0.000 | 0.000 | 0.017 | 0.220 | 0.000 | 0.010 | 0.012 | 0.000 | 0.000 | -0.019 | 0.040 | 0.000 | -0.002 | 0.000 | 0.000 | |||||||||||||
| D3 | 0.099 | 0.102 | 0.029 | 0.009 | 0.000 | 0.011 | 0.033 | 0.011 | 0.003 | 0.108 | 0.000 | 0.009 | 0.003 | 0.004 | 0.030 | 0.000 | 0.032 | 0.019 | 0.047 | 0.012 | 0.006 | 0.000 | ||||||||||||||
| D4 | 0.076 | 0.061 | 0.001 | 0.026 | -0.002 | -0.001 | 0.000 | 0.034 | 0.061 | 0.006 | 0.014 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.072 | 0.004 | 0.000 | |||||||||||||||
| D5 | 0.073 | 0.043 | 0.000 | 0.096 | 0.045 | 0.062 | 0.000 | 0.018 | 0.000 | 0.000 | 0.002 | 0.000 | 0.042 | 0.003 | 0.040 | 0.007 | 0.000 | 0.008 | 0.000 | 0.000 | ||||||||||||||||
| A1 | 0.012 | 0.014 | 0.065 | 0.074 | 0.034 | 0.061 | 0.003 | 0.032 | 0.042 | 0.022 | 0.000 | 0.043 | 0.015 | 0.015 | 0.093 | 0.000 | 0.050 | 0.000 | -0.002 | |||||||||||||||||
| A2 | 0.086 | 0.028 | 0.066 | 0.054 | 0.011 | 0.014 | 0.071 | 0.041 | 0.000 | 0.000 | 0.034 | 0.000 | 0.015 | 0.001 | 0.000 | 0.012 | 0.000 | 0.000 | ||||||||||||||||||
| A3 | 0.055 | 0.089 | 0.062 | 0.047 | 0.016 | 0.049 | 0.005 | 0.058 | 0.000 | 0.000 | 0.051 | 0.000 | 0.026 | -0.036 | 0.000 | -0.054 | -0.019 | |||||||||||||||||||
| A5 | 0.131 | 0.081 | 0.036 | 0.000 | 0.037 | -0.009 | 0.031 | 0.000 | 0.000 | 0.004 | 0.000 | 0.123 | 0.010 | -0.004 | 0.000 | -0.014 | ||||||||||||||||||||
| A6 | 0.140 | 0.020 | 0.024 | 0.017 | 0.029 | 0.059 | 0.038 | 0.060 | 0.111 | 0.000 | 0.014 | 0.000 | 0.000 | -0.041 | -0.019 | |||||||||||||||||||||
| A7 | 0.055 | 0.000 | 0.018 | 0.013 | 0.011 | 0.000 | 0.012 | 0.014 | 0.000 | 0.100 | -0.009 | 0.060 | 0.005 | 0.000 | ||||||||||||||||||||||
| A9 | 0.086 | 0.025 | 0.049 | 0.000 | 0.018 | 0.000 | 0.005 | 0.097 | 0.073 | -0.012 | 0.033 | 0.000 | 0.000 | |||||||||||||||||||||||
| A10 | 0.122 | -0.014 | 0.032 | 0.009 | 0.038 | 0.099 | 0.002 | 0.033 | 0.000 | 0.024 | -0.036 | 0.000 | ||||||||||||||||||||||||
| A11 | 0.037 | 0.000 | 0.042 | 0.021 | 0.036 | 0.000 | 0.000 | 0.000 | 0.018 | 0.000 | -0.036 | |||||||||||||||||||||||||
| A13 | 0.048 | 0.000 | 0.017 | 0.003 | 0.000 | 0.029 | 0.025 | 0.015 | 0.088 | 0.126 | ||||||||||||||||||||||||||
| A14 | 0.257 | 0.044 | 0.097 | 0.135 | 0.002 | -0.008 | 0.020 | -0.021 | -0.032 | |||||||||||||||||||||||||||
| A15 | 0.014 | 0.000 | 0.256 | 0.025 | 0.000 | 0.050 | 0.008 | -0.073 | ||||||||||||||||||||||||||||
| A17 | 0.462 | 0.098 | 0.010 | 0.017 | -0.023 | -0.037 | 0.000 | |||||||||||||||||||||||||||||
| A18 | 0.085 | 0.041 | 0.000 | 0.015 | -0.018 | 0.002 | ||||||||||||||||||||||||||||||
| A19 | 0.074 | -0.043 | 0.028 | 0.000 | -0.006 | |||||||||||||||||||||||||||||||
| A20 | 0.000 | 0.000 | 0.042 | 0.008 | ||||||||||||||||||||||||||||||||
| A4 | 0.101 | 0.139 | 0.258 | |||||||||||||||||||||||||||||||||
| A8 | 0.107 | 0.029 | ||||||||||||||||||||||||||||||||||
| A12 | 0.403 |
Table 1 The weight of each edge in Wenchuan Network (all symptoms)
| B2 | B3 | B4 | B5 | C1 | C2 | C3 | C4 | C5 | C6 | C7 | D1 | D2 | D3 | D4 | D5 | A1 | A2 | A3 | A5 | A6 | A7 | A9 | A10 | A11 | A13 | A14 | A15 | A17 | A18 | A19 | A20 | A4 | A8 | A12 | A16 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B1 | 0.094 | 0.036 | 0.010 | 0.035 | 0.000 | -0.009 | 0.050 | 0.000 | 0.002 | -0.035 | 0.078 | 0.000 | 0.175 | 0.075 | 0.001 | 0.034 | 0.000 | 0.022 | 0.007 | -0.003 | 0.002 | 0.000 | 0.000 | 0.137 | 0.054 | 0.000 | 0.000 | 0.025 | 0.000 | 0.000 | 0.005 | -0.018 | 0.000 | 0.016 | 0.004 | 0.000 |
| B2 | 0.172 | 0.171 | 0.057 | 0.000 | -0.009 | 0.128 | 0.031 | 0.000 | -0.011 | 0.076 | 0.032 | 0.000 | 0.068 | 0.061 | 0.011 | 0.000 | 0.007 | 0.000 | -0.010 | 0.000 | 0.000 | 0.000 | 0.070 | 0.026 | 0.010 | 0.000 | -0.009 | 0.008 | 0.020 | -0.005 | 0.000 | 0.048 | 0.000 | 0.000 | 0.005 | |
| B3 | 0.101 | 0.173 | 0.018 | 0.000 | 0.089 | 0.038 | -0.006 | -0.055 | 0.053 | 0.000 | 0.010 | 0.058 | 0.000 | 0.002 | 0.051 | 0.043 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.052 | 0.000 | 0.020 | -0.013 | -0.018 | 0.056 | 0.073 | -0.009 | 0.000 | 0.017 | -0.003 | 0.000 | 0.016 | ||
| B4 | 0.157 | 0.000 | 0.005 | 0.082 | 0.069 | 0.039 | 0.000 | 0.011 | 0.000 | 0.000 | 0.074 | 0.045 | 0.000 | 0.042 | 0.015 | 0.000 | 0.000 | 0.000 | 0.000 | 0.022 | 0.064 | 0.013 | 0.000 | -0.011 | 0.014 | 0.007 | 0.000 | 0.000 | 0.006 | 0.015 | 0.000 | -0.021 | 0.000 | |||
| B5 | 0.000 | 0.000 | 0.095 | 0.042 | 0.025 | -0.001 | 0.059 | 0.010 | 0.015 | 0.006 | 0.052 | 0.000 | 0.015 | 0.006 | 0.018 | 0.000 | 0.009 | 0.012 | 0.000 | 0.103 | 0.022 | 0.018 | -0.002 | 0.000 | 0.000 | 0.000 | -0.005 | 0.008 | -0.023 | 0.026 | 0.000 | -0.004 | ||||
| C1 | 0.050 | 0.069 | 0.029 | 0.015 | 0.061 | 0.049 | 0.073 | 0.066 | 0.013 | 0.006 | 0.024 | 0.047 | 0.010 | 0.006 | 0.024 | 0.047 | 0.016 | 0.040 | 0.000 | 0.000 | 0.036 | 0.000 | 0.000 | 0.000 | -0.009 | 0.000 | 0.041 | 0.000 | 0.000 | -0.012 | 0.000 | |||||
| C2 | 0.001 | 0.001 | 0.011 | 0.109 | -0.011 | 0.083 | 0.032 | 0.046 | 0.021 | 0.017 | 0.050 | 0.000 | 0.000 | 0.033 | 0.000 | 0.063 | 0.067 | 0.000 | 0.000 | 0.000 | 0.031 | 0.000 | -0.012 | 0.000 | 0.058 | 0.080 | 0.000 | -0.004 | -0.014 | -0.025 | ||||||
| C3 | 0.015 | 0.008 | 0.000 | 0.143 | 0.000 | 0.020 | 0.017 | 0.048 | -0.019 | 0.000 | -0.003 | 0.017 | -0.026 | 0.000 | 0.000 | 0.000 | 0.018 | 0.003 | 0.000 | 0.000 | 0.000 | 0.003 | 0.010 | 0.000 | 0.000 | -0.005 | 0.007 | 0.000 | 0.000 | |||||||
| C4 | 0.023 | 0.062 | 0.003 | 0.061 | 0.070 | 0.022 | 0.040 | 0.051 | 0.003 | 0.023 | 0.128 | 0.000 | 0.057 | 0.045 | 0.014 | 0.011 | 0.010 | 0.026 | 0.027 | 0.009 | 0.019 | 0.053 | 0.000 | 0.028 | 0.000 | 0.000 | 0.000 | -0.011 | ||||||||
| C5 | 0.069 | 0.055 | 0.002 | 0.000 | -0.016 | 0.037 | 0.036 | 0.010 | 0.010 | 0.048 | 0.000 | 0.000 | 0.024 | 0.000 | 0.039 | 0.005 | 0.014 | 0.000 | 0.031 | -0.004 | -0.036 | 0.000 | 0.056 | 0.000 | 0.009 | 0.015 | 0.007 | |||||||||
| C6 | 0.000 | 0.021 | 0.009 | 0.023 | 0.024 | 0.150 | 0.003 | 0.000 | 0.058 | 0.012 | 0.045 | 0.045 | 0.042 | -0.034 | 0.018 | 0.037 | 0.141 | 0.066 | 0.000 | 0.001 | 0.118 | 0.065 | -0.001 | 0.000 | -0.009 | 0.000 | ||||||||||
| C7 | 0.019 | 0.000 | 0.000 | 0.048 | 0.000 | 0.000 | 0.041 | 0.055 | -0.005 | -0.004 | 0.000 | 0.046 | 0.003 | 0.000 | 0.006 | -0.007 | 0.000 | 0.000 | -0.002 | 0.000 | 0.020 | 0.000 | 0.020 | 0.000 | 0.032 | |||||||||||
| D1 | 0.109 | 0.013 | 0.000 | 0.043 | 0.010 | 0.000 | 0.000 | 0.295 | 0.029 | 0.003 | 0.055 | 0.010 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.039 | 0.000 | 0.000 | -0.033 | 0.000 | ||||||||||||
| D2 | 0.047 | 0.047 | 0.004 | 0.000 | 0.042 | 0.000 | 0.051 | 0.000 | 0.000 | 0.000 | 0.017 | 0.220 | 0.000 | 0.010 | 0.012 | 0.000 | 0.000 | -0.019 | 0.040 | 0.000 | -0.002 | 0.000 | 0.000 | |||||||||||||
| D3 | 0.099 | 0.102 | 0.029 | 0.009 | 0.000 | 0.011 | 0.033 | 0.011 | 0.003 | 0.108 | 0.000 | 0.009 | 0.003 | 0.004 | 0.030 | 0.000 | 0.032 | 0.019 | 0.047 | 0.012 | 0.006 | 0.000 | ||||||||||||||
| D4 | 0.076 | 0.061 | 0.001 | 0.026 | -0.002 | -0.001 | 0.000 | 0.034 | 0.061 | 0.006 | 0.014 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.072 | 0.004 | 0.000 | |||||||||||||||
| D5 | 0.073 | 0.043 | 0.000 | 0.096 | 0.045 | 0.062 | 0.000 | 0.018 | 0.000 | 0.000 | 0.002 | 0.000 | 0.042 | 0.003 | 0.040 | 0.007 | 0.000 | 0.008 | 0.000 | 0.000 | ||||||||||||||||
| A1 | 0.012 | 0.014 | 0.065 | 0.074 | 0.034 | 0.061 | 0.003 | 0.032 | 0.042 | 0.022 | 0.000 | 0.043 | 0.015 | 0.015 | 0.093 | 0.000 | 0.050 | 0.000 | -0.002 | |||||||||||||||||
| A2 | 0.086 | 0.028 | 0.066 | 0.054 | 0.011 | 0.014 | 0.071 | 0.041 | 0.000 | 0.000 | 0.034 | 0.000 | 0.015 | 0.001 | 0.000 | 0.012 | 0.000 | 0.000 | ||||||||||||||||||
| A3 | 0.055 | 0.089 | 0.062 | 0.047 | 0.016 | 0.049 | 0.005 | 0.058 | 0.000 | 0.000 | 0.051 | 0.000 | 0.026 | -0.036 | 0.000 | -0.054 | -0.019 | |||||||||||||||||||
| A5 | 0.131 | 0.081 | 0.036 | 0.000 | 0.037 | -0.009 | 0.031 | 0.000 | 0.000 | 0.004 | 0.000 | 0.123 | 0.010 | -0.004 | 0.000 | -0.014 | ||||||||||||||||||||
| A6 | 0.140 | 0.020 | 0.024 | 0.017 | 0.029 | 0.059 | 0.038 | 0.060 | 0.111 | 0.000 | 0.014 | 0.000 | 0.000 | -0.041 | -0.019 | |||||||||||||||||||||
| A7 | 0.055 | 0.000 | 0.018 | 0.013 | 0.011 | 0.000 | 0.012 | 0.014 | 0.000 | 0.100 | -0.009 | 0.060 | 0.005 | 0.000 | ||||||||||||||||||||||
| A9 | 0.086 | 0.025 | 0.049 | 0.000 | 0.018 | 0.000 | 0.005 | 0.097 | 0.073 | -0.012 | 0.033 | 0.000 | 0.000 | |||||||||||||||||||||||
| A10 | 0.122 | -0.014 | 0.032 | 0.009 | 0.038 | 0.099 | 0.002 | 0.033 | 0.000 | 0.024 | -0.036 | 0.000 | ||||||||||||||||||||||||
| A11 | 0.037 | 0.000 | 0.042 | 0.021 | 0.036 | 0.000 | 0.000 | 0.000 | 0.018 | 0.000 | -0.036 | |||||||||||||||||||||||||
| A13 | 0.048 | 0.000 | 0.017 | 0.003 | 0.000 | 0.029 | 0.025 | 0.015 | 0.088 | 0.126 | ||||||||||||||||||||||||||
| A14 | 0.257 | 0.044 | 0.097 | 0.135 | 0.002 | -0.008 | 0.020 | -0.021 | -0.032 | |||||||||||||||||||||||||||
| A15 | 0.014 | 0.000 | 0.256 | 0.025 | 0.000 | 0.050 | 0.008 | -0.073 | ||||||||||||||||||||||||||||
| A17 | 0.462 | 0.098 | 0.010 | 0.017 | -0.023 | -0.037 | 0.000 | |||||||||||||||||||||||||||||
| A18 | 0.085 | 0.041 | 0.000 | 0.015 | -0.018 | 0.002 | ||||||||||||||||||||||||||||||
| A19 | 0.074 | -0.043 | 0.028 | 0.000 | -0.006 | |||||||||||||||||||||||||||||||
| A20 | 0.000 | 0.000 | 0.042 | 0.008 | ||||||||||||||||||||||||||||||||
| A4 | 0.101 | 0.139 | 0.258 | |||||||||||||||||||||||||||||||||
| A8 | 0.107 | 0.029 | ||||||||||||||||||||||||||||||||||
| A12 | 0.403 |
| B2 | B3 | B4 | B5 | C1 | C2 | C3 | C4 | C5 | C6 | C7 | D1 | D2 | D3 | D4 | D5 | A1 | A2 | A3 | A5 | A6 | A7 | A9 | A10 | A11 | A13 | A14 | A15 | A17 | A18 | A19 | A20 | A4 | A8 | A12 | A16 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B1 | 0.094 | 0.011 | 0.010 | 0.035 | 0.000 | -0.009 | 0.050 | 0.000 | 0.000 | 0.000 | 0.078 | 0.000 | 0.175 | 0.075 | 0.001 | 0.034 | 0.000 | 0.022 | 0.007 | -0.003 | 0.002 | 0.000 | 0.000 | 0.137 | 0.054 | 0.000 | 0.000 | 0.025 | 0.000 | 0.007 | 0.005 | -0.018 | 0.000 | 0.016 | 0.000 | 0.000 |
| B2 | 0.172 | 0.171 | 0.057 | 0.000 | -0.007 | 0.128 | 0.031 | 0.000 | -0.011 | 0.076 | 0.000 | 0.000 | 0.068 | 0.061 | 0.011 | 0.000 | 0.007 | 0.000 | -0.010 | 0.000 | 0.000 | 0.000 | 0.070 | 0.026 | 0.006 | 0.000 | 0.000 | 0.004 | 0.020 | 0.009 | 0.000 | 0.039 | 0.000 | 0.000 | 0.000 | |
| B3 | 0.101 | 0.174 | 0.018 | 0.000 | 0.089 | 0.038 | 0.000 | -0.055 | 0.053 | 0.000 | 0.010 | 0.058 | 0.000 | 0.002 | 0.051 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.052 | 0.000 | 0.020 | -0.013 | -0.018 | 0.056 | 0.073 | 0.000 | 0.000 | 0.017 | -0.003 | 0.000 | 0.000 | ||
| B4 | 0.157 | 0.000 | 0.005 | 0.144 | 0.062 | 0.000 | 0.000 | 0.011 | 0.000 | 0.000 | 0.074 | 0.045 | 0.000 | 0.042 | 0.015 | 0.000 | 0.000 | 0.000 | 0.000 | 0.011 | 0.064 | 0.000 | 0.000 | -0.011 | 0.014 | 0.007 | 0.000 | 0.000 | 0.006 | 0.000 | 0.000 | -0.028 | 0.000 | |||
| B5 | 0.000 | 0.000 | 0.095 | 0.042 | 0.025 | -0.001 | 0.059 | 0.010 | 0.015 | 0.040 | 0.052 | 0.000 | 0.015 | 0.000 | 0.018 | 0.000 | 0.000 | 0.012 | 0.000 | 0.103 | 0.022 | 0.018 | -0.002 | 0.000 | 0.000 | 0.000 | -0.005 | 0.008 | -0.023 | 0.026 | 0.000 | -0.004 | ||||
| C1 | 0.050 | 0.069 | 0.029 | 0.004 | 0.061 | 0.045 | 0.073 | 0.059 | 0.013 | 0.001 | 0.024 | 0.047 | 0.010 | 0.016 | 0.053 | 0.047 | 0.016 | 0.040 | 0.000 | 0.000 | 0.036 | 0.000 | 0.000 | 0.000 | -0.009 | 0.000 | 0.041 | 0.000 | 0.000 | -0.012 | 0.000 | |||||
| C2 | 0.001 | 0.001 | 0.014 | 0.109 | -0.011 | 0.083 | 0.032 | 0.046 | 0.021 | 0.017 | 0.050 | 0.000 | 0.000 | 0.033 | 0.000 | 0.063 | 0.067 | 0.000 | 0.000 | 0.000 | 0.031 | 0.000 | -0.006 | 0.000 | 0.058 | 0.080 | 0.000 | -0.004 | -0.014 | -0.031 | ||||||
| C3 | 0.015 | 0.000 | 0.000 | 0.143 | 0.000 | 0.020 | 0.017 | 0.048 | -0.019 | 0.000 | -0.003 | 0.017 | -0.026 | 0.000 | 0.000 | 0.000 | 0.027 | 0.003 | 0.000 | 0.000 | 0.000 | 0.003 | 0.010 | 0.000 | 0.000 | -0.005 | 0.007 | 0.000 | 0.000 | |||||||
| C4 | 0.023 | 0.062 | 0.003 | 0.061 | 0.070 | 0.022 | 0.040 | 0.051 | 0.003 | 0.023 | 0.128 | 0.000 | 0.057 | 0.045 | 0.014 | 0.010 | 0.010 | 0.060 | 0.027 | 0.009 | 0.019 | 0.053 | 0.000 | 0.028 | 0.000 | 0.000 | 0.000 | -0.011 | ||||||||
| C5 | 0.021 | 0.055 | 0.002 | 0.000 | -0.001 | 0.020 | 0.036 | 0.010 | 0.010 | 0.048 | 0.000 | 0.000 | 0.024 | 0.014 | 0.039 | 0.005 | 0.009 | 0.000 | 0.031 | -0.004 | -0.036 | 0.000 | 0.056 | 0.000 | 0.000 | 0.000 | 0.000 | |||||||||
| C6 | 0.000 | 0.021 | 0.009 | 0.023 | 0.012 | 0.150 | 0.003 | 0.000 | 0.058 | 0.012 | 0.045 | 0.045 | 0.042 | -0.034 | 0.018 | 0.037 | 0.141 | 0.066 | 0.000 | 0.001 | 0.118 | 0.052 | -0.001 | 0.000 | -0.009 | -0.015 | ||||||||||
| C7 | 0.000 | 0.000 | 0.000 | 0.048 | 0.000 | 0.000 | 0.041 | 0.055 | -0.005 | -0.004 | 0.000 | 0.017 | 0.003 | 0.000 | 0.006 | -0.007 | 0.000 | 0.000 | -0.002 | 0.000 | 0.020 | 0.000 | 0.020 | 0.000 | 0.000 | |||||||||||
| D1 | 0.060 | 0.013 | 0.000 | 0.043 | 0.010 | 0.000 | 0.000 | 0.295 | 0.040 | 0.003 | 0.055 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.039 | -0.018 | -0.028 | -0.033 | 0.000 | ||||||||||||
| D2 | 0.047 | 0.047 | 0.004 | 0.000 | 0.042 | 0.000 | 0.051 | 0.000 | 0.000 | 0.000 | 0.017 | 0.236 | 0.000 | 0.010 | 0.012 | 0.000 | 0.000 | 0.000 | 0.040 | 0.000 | -0.002 | 0.000 | 0.000 | |||||||||||||
| D3 | 0.099 | 0.102 | 0.029 | 0.009 | 0.000 | 0.000 | 0.033 | 0.011 | 0.003 | 0.108 | 0.000 | 0.000 | 0.003 | 0.004 | 0.030 | 0.000 | 0.032 | 0.000 | 0.000 | 0.012 | 0.000 | 0.000 | ||||||||||||||
| D4 | 0.076 | 0.045 | 0.001 | 0.026 | -0.002 | -0.001 | 0.000 | 0.034 | 0.061 | 0.013 | 0.014 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.045 | 0.003 | 0.000 | |||||||||||||||
| D5 | 0.042 | 0.043 | 0.000 | 0.096 | 0.045 | 0.062 | 0.000 | 0.018 | 0.000 | 0.000 | 0.000 | 0.000 | 0.042 | 0.003 | 0.040 | 0.006 | 0.000 | 0.008 | 0.000 | 0.000 | ||||||||||||||||
| A1 | 0.012 | 0.042 | 0.065 | 0.074 | 0.034 | 0.061 | 0.003 | 0.032 | 0.042 | 0.022 | 0.000 | 0.043 | 0.015 | 0.015 | 0.118 | 0.000 | 0.000 | 0.000 | -0.002 | |||||||||||||||||
| A2 | 0.086 | 0.028 | 0.066 | 0.054 | 0.011 | 0.014 | 0.071 | 0.041 | 0.000 | 0.000 | 0.033 | 0.000 | 0.015 | 0.001 | 0.000 | 0.012 | 0.000 | 0.000 | ||||||||||||||||||
| A3 | 0.055 | 0.078 | 0.062 | 0.047 | 0.016 | 0.049 | 0.005 | 0.058 | 0.000 | 0.000 | 0.051 | 0.000 | 0.026 | -0.036 | 0.000 | -0.054 | -0.019 | |||||||||||||||||||
| A5 | 0.131 | 0.081 | 0.047 | 0.000 | 0.037 | -0.006 | 0.031 | 0.000 | 0.000 | 0.004 | 0.000 | 0.123 | 0.010 | -0.004 | 0.000 | -0.014 | ||||||||||||||||||||
| A6 | 0.140 | 0.020 | 0.024 | 0.017 | 0.029 | 0.059 | 0.038 | 0.060 | 0.111 | 0.000 | 0.000 | 0.000 | 0.000 | -0.041 | -0.019 | |||||||||||||||||||||
| A7 | 0.055 | 0.000 | 0.018 | 0.013 | 0.011 | 0.000 | 0.012 | 0.014 | 0.000 | 0.100 | -0.009 | 0.056 | -0.021 | 0.000 | ||||||||||||||||||||||
| A9 | 0.086 | 0.025 | 0.049 | 0.000 | 0.018 | 0.000 | 0.017 | 0.097 | 0.073 | -0.012 | 0.033 | -0.042 | 0.000 | |||||||||||||||||||||||
| A10 | 0.123 | -0.014 | 0.032 | 0.009 | 0.038 | 0.099 | 0.002 | 0.033 | 0.000 | 0.000 | -0.036 | 0.000 | ||||||||||||||||||||||||
| A11 | 0.037 | 0.000 | 0.031 | 0.021 | 0.036 | 0.000 | 0.000 | 0.000 | 0.006 | -0.006 | -0.036 | |||||||||||||||||||||||||
| A13 | 0.048 | 0.000 | 0.017 | 0.003 | 0.000 | 0.029 | 0.025 | 0.015 | 0.084 | 0.045 | ||||||||||||||||||||||||||
| A14 | 0.257 | 0.044 | 0.097 | 0.135 | 0.002 | -0.008 | 0.000 | -0.021 | -0.032 | |||||||||||||||||||||||||||
| A15 | 0.014 | 0.000 | 0.256 | 0.019 | 0.000 | 0.050 | 0.000 | -0.073 | ||||||||||||||||||||||||||||
| A17 | 0.462 | 0.098 | 0.010 | 0.017 | -0.023 | -0.037 | 0.000 | |||||||||||||||||||||||||||||
| A18 | 0.085 | 0.041 | 0.000 | 0.000 | -0.018 | -0.011 | ||||||||||||||||||||||||||||||
| A19 | 0.074 | -0.043 | 0.022 | 0.000 | -0.027 | |||||||||||||||||||||||||||||||
| A20 | 0.000 | 0.000 | 0.037 | 0.008 | ||||||||||||||||||||||||||||||||
| A4 | 0.126 | 0.138 | 0.257 | |||||||||||||||||||||||||||||||||
| A8 | 0.106 | 0.032 | ||||||||||||||||||||||||||||||||||
| A12 | 0.399 |
Table 2 The weight of each edge in Ya'an Network (all symptoms)
| B2 | B3 | B4 | B5 | C1 | C2 | C3 | C4 | C5 | C6 | C7 | D1 | D2 | D3 | D4 | D5 | A1 | A2 | A3 | A5 | A6 | A7 | A9 | A10 | A11 | A13 | A14 | A15 | A17 | A18 | A19 | A20 | A4 | A8 | A12 | A16 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B1 | 0.094 | 0.011 | 0.010 | 0.035 | 0.000 | -0.009 | 0.050 | 0.000 | 0.000 | 0.000 | 0.078 | 0.000 | 0.175 | 0.075 | 0.001 | 0.034 | 0.000 | 0.022 | 0.007 | -0.003 | 0.002 | 0.000 | 0.000 | 0.137 | 0.054 | 0.000 | 0.000 | 0.025 | 0.000 | 0.007 | 0.005 | -0.018 | 0.000 | 0.016 | 0.000 | 0.000 |
| B2 | 0.172 | 0.171 | 0.057 | 0.000 | -0.007 | 0.128 | 0.031 | 0.000 | -0.011 | 0.076 | 0.000 | 0.000 | 0.068 | 0.061 | 0.011 | 0.000 | 0.007 | 0.000 | -0.010 | 0.000 | 0.000 | 0.000 | 0.070 | 0.026 | 0.006 | 0.000 | 0.000 | 0.004 | 0.020 | 0.009 | 0.000 | 0.039 | 0.000 | 0.000 | 0.000 | |
| B3 | 0.101 | 0.174 | 0.018 | 0.000 | 0.089 | 0.038 | 0.000 | -0.055 | 0.053 | 0.000 | 0.010 | 0.058 | 0.000 | 0.002 | 0.051 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.052 | 0.000 | 0.020 | -0.013 | -0.018 | 0.056 | 0.073 | 0.000 | 0.000 | 0.017 | -0.003 | 0.000 | 0.000 | ||
| B4 | 0.157 | 0.000 | 0.005 | 0.144 | 0.062 | 0.000 | 0.000 | 0.011 | 0.000 | 0.000 | 0.074 | 0.045 | 0.000 | 0.042 | 0.015 | 0.000 | 0.000 | 0.000 | 0.000 | 0.011 | 0.064 | 0.000 | 0.000 | -0.011 | 0.014 | 0.007 | 0.000 | 0.000 | 0.006 | 0.000 | 0.000 | -0.028 | 0.000 | |||
| B5 | 0.000 | 0.000 | 0.095 | 0.042 | 0.025 | -0.001 | 0.059 | 0.010 | 0.015 | 0.040 | 0.052 | 0.000 | 0.015 | 0.000 | 0.018 | 0.000 | 0.000 | 0.012 | 0.000 | 0.103 | 0.022 | 0.018 | -0.002 | 0.000 | 0.000 | 0.000 | -0.005 | 0.008 | -0.023 | 0.026 | 0.000 | -0.004 | ||||
| C1 | 0.050 | 0.069 | 0.029 | 0.004 | 0.061 | 0.045 | 0.073 | 0.059 | 0.013 | 0.001 | 0.024 | 0.047 | 0.010 | 0.016 | 0.053 | 0.047 | 0.016 | 0.040 | 0.000 | 0.000 | 0.036 | 0.000 | 0.000 | 0.000 | -0.009 | 0.000 | 0.041 | 0.000 | 0.000 | -0.012 | 0.000 | |||||
| C2 | 0.001 | 0.001 | 0.014 | 0.109 | -0.011 | 0.083 | 0.032 | 0.046 | 0.021 | 0.017 | 0.050 | 0.000 | 0.000 | 0.033 | 0.000 | 0.063 | 0.067 | 0.000 | 0.000 | 0.000 | 0.031 | 0.000 | -0.006 | 0.000 | 0.058 | 0.080 | 0.000 | -0.004 | -0.014 | -0.031 | ||||||
| C3 | 0.015 | 0.000 | 0.000 | 0.143 | 0.000 | 0.020 | 0.017 | 0.048 | -0.019 | 0.000 | -0.003 | 0.017 | -0.026 | 0.000 | 0.000 | 0.000 | 0.027 | 0.003 | 0.000 | 0.000 | 0.000 | 0.003 | 0.010 | 0.000 | 0.000 | -0.005 | 0.007 | 0.000 | 0.000 | |||||||
| C4 | 0.023 | 0.062 | 0.003 | 0.061 | 0.070 | 0.022 | 0.040 | 0.051 | 0.003 | 0.023 | 0.128 | 0.000 | 0.057 | 0.045 | 0.014 | 0.010 | 0.010 | 0.060 | 0.027 | 0.009 | 0.019 | 0.053 | 0.000 | 0.028 | 0.000 | 0.000 | 0.000 | -0.011 | ||||||||
| C5 | 0.021 | 0.055 | 0.002 | 0.000 | -0.001 | 0.020 | 0.036 | 0.010 | 0.010 | 0.048 | 0.000 | 0.000 | 0.024 | 0.014 | 0.039 | 0.005 | 0.009 | 0.000 | 0.031 | -0.004 | -0.036 | 0.000 | 0.056 | 0.000 | 0.000 | 0.000 | 0.000 | |||||||||
| C6 | 0.000 | 0.021 | 0.009 | 0.023 | 0.012 | 0.150 | 0.003 | 0.000 | 0.058 | 0.012 | 0.045 | 0.045 | 0.042 | -0.034 | 0.018 | 0.037 | 0.141 | 0.066 | 0.000 | 0.001 | 0.118 | 0.052 | -0.001 | 0.000 | -0.009 | -0.015 | ||||||||||
| C7 | 0.000 | 0.000 | 0.000 | 0.048 | 0.000 | 0.000 | 0.041 | 0.055 | -0.005 | -0.004 | 0.000 | 0.017 | 0.003 | 0.000 | 0.006 | -0.007 | 0.000 | 0.000 | -0.002 | 0.000 | 0.020 | 0.000 | 0.020 | 0.000 | 0.000 | |||||||||||
| D1 | 0.060 | 0.013 | 0.000 | 0.043 | 0.010 | 0.000 | 0.000 | 0.295 | 0.040 | 0.003 | 0.055 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.039 | -0.018 | -0.028 | -0.033 | 0.000 | ||||||||||||
| D2 | 0.047 | 0.047 | 0.004 | 0.000 | 0.042 | 0.000 | 0.051 | 0.000 | 0.000 | 0.000 | 0.017 | 0.236 | 0.000 | 0.010 | 0.012 | 0.000 | 0.000 | 0.000 | 0.040 | 0.000 | -0.002 | 0.000 | 0.000 | |||||||||||||
| D3 | 0.099 | 0.102 | 0.029 | 0.009 | 0.000 | 0.000 | 0.033 | 0.011 | 0.003 | 0.108 | 0.000 | 0.000 | 0.003 | 0.004 | 0.030 | 0.000 | 0.032 | 0.000 | 0.000 | 0.012 | 0.000 | 0.000 | ||||||||||||||
| D4 | 0.076 | 0.045 | 0.001 | 0.026 | -0.002 | -0.001 | 0.000 | 0.034 | 0.061 | 0.013 | 0.014 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.045 | 0.003 | 0.000 | |||||||||||||||
| D5 | 0.042 | 0.043 | 0.000 | 0.096 | 0.045 | 0.062 | 0.000 | 0.018 | 0.000 | 0.000 | 0.000 | 0.000 | 0.042 | 0.003 | 0.040 | 0.006 | 0.000 | 0.008 | 0.000 | 0.000 | ||||||||||||||||
| A1 | 0.012 | 0.042 | 0.065 | 0.074 | 0.034 | 0.061 | 0.003 | 0.032 | 0.042 | 0.022 | 0.000 | 0.043 | 0.015 | 0.015 | 0.118 | 0.000 | 0.000 | 0.000 | -0.002 | |||||||||||||||||
| A2 | 0.086 | 0.028 | 0.066 | 0.054 | 0.011 | 0.014 | 0.071 | 0.041 | 0.000 | 0.000 | 0.033 | 0.000 | 0.015 | 0.001 | 0.000 | 0.012 | 0.000 | 0.000 | ||||||||||||||||||
| A3 | 0.055 | 0.078 | 0.062 | 0.047 | 0.016 | 0.049 | 0.005 | 0.058 | 0.000 | 0.000 | 0.051 | 0.000 | 0.026 | -0.036 | 0.000 | -0.054 | -0.019 | |||||||||||||||||||
| A5 | 0.131 | 0.081 | 0.047 | 0.000 | 0.037 | -0.006 | 0.031 | 0.000 | 0.000 | 0.004 | 0.000 | 0.123 | 0.010 | -0.004 | 0.000 | -0.014 | ||||||||||||||||||||
| A6 | 0.140 | 0.020 | 0.024 | 0.017 | 0.029 | 0.059 | 0.038 | 0.060 | 0.111 | 0.000 | 0.000 | 0.000 | 0.000 | -0.041 | -0.019 | |||||||||||||||||||||
| A7 | 0.055 | 0.000 | 0.018 | 0.013 | 0.011 | 0.000 | 0.012 | 0.014 | 0.000 | 0.100 | -0.009 | 0.056 | -0.021 | 0.000 | ||||||||||||||||||||||
| A9 | 0.086 | 0.025 | 0.049 | 0.000 | 0.018 | 0.000 | 0.017 | 0.097 | 0.073 | -0.012 | 0.033 | -0.042 | 0.000 | |||||||||||||||||||||||
| A10 | 0.123 | -0.014 | 0.032 | 0.009 | 0.038 | 0.099 | 0.002 | 0.033 | 0.000 | 0.000 | -0.036 | 0.000 | ||||||||||||||||||||||||
| A11 | 0.037 | 0.000 | 0.031 | 0.021 | 0.036 | 0.000 | 0.000 | 0.000 | 0.006 | -0.006 | -0.036 | |||||||||||||||||||||||||
| A13 | 0.048 | 0.000 | 0.017 | 0.003 | 0.000 | 0.029 | 0.025 | 0.015 | 0.084 | 0.045 | ||||||||||||||||||||||||||
| A14 | 0.257 | 0.044 | 0.097 | 0.135 | 0.002 | -0.008 | 0.000 | -0.021 | -0.032 | |||||||||||||||||||||||||||
| A15 | 0.014 | 0.000 | 0.256 | 0.019 | 0.000 | 0.050 | 0.000 | -0.073 | ||||||||||||||||||||||||||||
| A17 | 0.462 | 0.098 | 0.010 | 0.017 | -0.023 | -0.037 | 0.000 | |||||||||||||||||||||||||||||
| A18 | 0.085 | 0.041 | 0.000 | 0.000 | -0.018 | -0.011 | ||||||||||||||||||||||||||||||
| A19 | 0.074 | -0.043 | 0.022 | 0.000 | -0.027 | |||||||||||||||||||||||||||||||
| A20 | 0.000 | 0.000 | 0.037 | 0.008 | ||||||||||||||||||||||||||||||||
| A4 | 0.126 | 0.138 | 0.257 | |||||||||||||||||||||||||||||||||
| A8 | 0.106 | 0.032 | ||||||||||||||||||||||||||||||||||
| A12 | 0.399 |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||