

1 引言
近年来, 新兴的行为治疗“第三浪潮”备受关注。行为治疗被喻为“第一浪潮”, 它基于条件反射和新行为原则, 直接关注有问题的行为和情绪; “第二浪潮”则强调对非理性思维、病理性认知图式或错误的信息处理方式进行矫正, 进而减轻或消除症状, 这种以认知改变为重心的治疗被称为“认知行为疗法” (Cognitive-Behavior Therapy, CBT) (Beck, 1993)。“第三浪潮”则对心理现象的语境和功能更为敏感, 而不仅仅关注其形式(Hayes, Luoma, Bond, Masuda, & Lillis, 2006), 典型的疗法包括接纳与承诺疗法(Acceptance and Commitment Therapy, ACT)、辩证行为疗法(Dialectical Behavioral Therapy, DBT)、正念认知疗法(Mindfulness Based Cognitive Therapy, MBCT)、慈悲聚焦疗法(Compassion Focused Therapy, CFT)等(Hacker, Stone, & MacBeth, 2016)。
尽管研究者们对哪些疗法属于“第三浪潮”仍存在争议, 但为了促进疗法的共同发展, 共识多于分歧。Hayes, Villatte, Levin和Hildebrandt (2011)对“第三浪潮”进行了修正, 用“基于语境的认知行为治疗” (Contextual Cognitive Behavioral Therapy, CCBT)作统称, 将关注点从原来的哪些治疗方法应该被纳入“第三浪潮”, 转为强调新兴疗法在理论、治疗过程和程序上“开放, 主动和觉察”的特点。在这些基于语境的认知行为治疗中, ACT最受关注, 近年来被引用的频次最多(Dimidjian et al., 2016)。本研究的目的在于系统考察ACT的作用机制, 相较之传统CBT的特异性, 以及在网络环境中的可迁移性。
1.1 ACT的疗效
探索ACT治疗的作用机制之前, 需要先考察其有效性。在循证心理治疗中, 随机对照试验(Randomized Controlled Trial, RCT)设计被作为疗法评估的“黄金标准”, 元分析证据被当作证据效度的最高标准(Wampold & Imel, 2015)。通常, 疗效有绝对疗效和相对疗效之分, 绝对疗效旨在检验该疗法是否有效, 其对照组一般是等待组(Waiting List, WL)、常规治疗(Treatment as Usual, TAU)、安慰剂治疗等; 相对疗效用于检验该疗法是否比其他疗法更为有效, 其对照组通常是高度结构化已确立的疗法, 比如传统CBT、认知疗法(Cognitive Therapy, CT)、人本主义疗法等(Wampold, 2013)。那么, ACT的疗效如何呢?
一方面, 从绝对疗效角度, 元分析的结果支持ACT具有中到大的效果量。最早的元分析纳入9篇RCT, 对照组包括WL、TAU、心理安慰剂组, 结果发现, ACT后测具有中等效果量(d = 0.66) (Hayes, et al., 2006); 最近一项纳入60项RCT研究的元分析(Öst, 2014)包括了更为广泛的心理、身体和工作压力相关问题, 相较之WL (g = 0.63)、TAU (g = 0.55)和心理安慰剂组(g = 0.59), 其后测的绝对疗效都具有中到大的效果量。
另一方面, 从相对疗效角度, 与高度结构化已确立的疗法对比, ACT的效果量大小不一。最早的元分析发现(Hayes et al., 2006)相较之传统CBT和CT, ACT具有中到大的效果量(d = 0.73), 但该研究只纳入了4项RCT研究。随后, Ruiz (2012)的元分析纳入16项RCT研究, 包括成瘾、慢性疼痛、焦虑症、抑郁症、压力以及癌症的心理体验等, 结果发现与传统CBT相比, ACT的后测(g = 0.37; g = 0.42)和追踪效果量都为小到中等, 之后更大样本的RCT研究(Öst, 2014)发现其后测效果量较小(k = 60, g = 0.16)。最近, 一项纳入39项RCT研究的元分析也得到类似的结果, 这项研究将治疗限定为临床相关疾病, 其干预中80%的成分包含ACT (A-Tjak et al., 2015)。
综上可见, 检验ACT的绝对疗效的元分析表明 ACT是有效的, 那么ACT是如何有效的, 即其作用机制值得进一步探究。
1.2 心理治疗机制的研究方法
机制是指解释改变过程, 而识别中介变量是检验作用机制的重要一步, 它是在统计上解释自变量与因变量关系的中间变量, 解释治疗为何和通过哪种方式作用于效果(MacKinnon, Fairchild, & Fritz, 2007)。
Kazdin (2007)归纳了识别心理治疗机制或中介变量的基本标准。首先, 研究中所提出的机制/中介变量和预期结果变量有明确的关联(强相关性准则)。其次, 结果变量和中介变量需要在多个时间点进行测量, 从而可以确定中介变量的变化先于结果变量的变化(时间优先准则)。再次, 需要操作实验设计(增加或减少特定机制), 激活和(或)拆除特定机制来确定效应的特异性(特异性准则)。此外, 需要观察“剂量-反应”关系, 即针对性地激活越多的机制剂量, 观察结果是否改变越强(梯度准则)。最后, 研究结果的可重复性(一致性标准)。
具体到统计上, 确立一个中介变量需要诸多条件。在很长一段时间, 中介仅指统计上的中介, 即从统计上证明治疗(X)对结果(Y)的影响可以通过第三变量(中介变量M)所解释。中介分析的方法众多, 显变量检验通常基于线性回归模型, 而潜变量检验则使用结构方程模型(Structural Equation Modeling, SEM)。虽然SEM技术相较之线性回归更具优势, 且研究者也更为推荐, 然而, 现今心理治疗研究中的中介检验, 传统线性回归法仍然是最为流行的方法(Gu, Strauss, Bond, & Cavanagh, 2015)。其中, 检验中介最经典的方法是逐步检验法(Baron & Kenny, 1986), 根据该方法, 治疗研究中介变量的确立需要满足以下几个条件(Lemmens, Müller, Arntz, & Huibers, 2016): (1)存在治疗主效应(疗效检验); (2)治疗与中介变量的改变相关(干预检验); (3)中介变量的改变和结果变量的改变相关(心理病理学检验); (4)当在统计上加入中介变量检验时, 治疗的效果不显著(完全中介)或显著性降低(部分中介)。
统计上的中介检验固然重要, 但鉴别治疗的中介变量仍需要一些额外的实验设计。根据较新的标准, 中介变量的鉴别需要建立在理论基础上, 通过严格的RCT, 进行合理间隔的重复测量, 并且要求有足够的统计力和合适的对照组(Kazdin, 2007; MacKinnon et al., 2007); 接着, 需要改进实验设计, 能在治疗研究中操作所提出的中介变量(Alsubaie et al., 2017); 此外, 根据治疗理论对改变过程的界定, 通常评价单一的中介变量是不足够的, 研究者推荐应该包括多个中介变量竞争假设, 检验替代解释模型, 并考察理论上中介变量之间的相互作用(Lemmens et al., 2016)。
1.3 ACT的作用机制
ACT基于关系框架理论, 其治疗机制模型假设是以提升心理灵活性为核心, 包括6大成分, 即, 接纳(愿意接触内心体验)、解离(将认知体验为持续的过程, 而非认知过度调节行为)、以已为景(把内在体验作为自身体验的背景, 而不把它看作是体验本身)、此时此刻(能够灵活地接触发生的内部与外部事件, 不作评判)、价值(选择持续行为模式所需的结果, 以建立强化物)、承诺行动(灵活地朝有价值的方向作出行动) (Hayes et al., 2006; 曾祥龙, 刘翔平, 于是, 2011; 张婍, 王淑娟, 祝卓宏, 2012)。上述机制假设是否能得到实证研究支持?
其一, 目前对ACT的治疗机制模型的实证检验结果存在不一致。部分研究验证了心理灵活性的改变在临床结果中起中介作用(Wicksell et al., 2013); 有的研究结果并不一致, 比如无法检验到对疼痛的接纳改变在实验条件组与追踪临床结果之间起部分或完全中介作用(Luciano et al., 2014); 再有研究发现, 在社区环境, ACT六边形模式的心理灵活性及6大核心机制的改变对焦虑障碍的改变作用是不一致的(Forman, Herbert, Moitra, Yeomans, & Geller, 2007; Hayes et al., 2006)。有元分析(Bluett, Homan, Morrison, Levin, & Twohig, 2014)考察63个检验焦虑与心理灵活性关系的研究, 结果显示, 二者在临床与非临床样本, 都具有中等程度的相关, 即, 在中等程度上支持心理灵活性是治疗改变的中介变量的可能。但不难看出, 该元分析仅是检验了心理灵活性与症状降低之间的相关性, 并没有直接检验中介作用。那么, 聚合所有相关研究进行中介检验, 是否能支持ACT的治疗机制模型?
其二, ACT所假设的作用机制是否具有特异性?ACT疗法在创始就强调其机制的独特性。Hayes(2004)认为, 相较之“第二浪潮”的传统CBT, 虽然“第三浪潮”与传统CBT有相同的干预成分, 比如自我监控、暴露和反应阻止法, 但二者在理论假设和干预方法都有所区别。在理论假设上, 区别于传统CBT, ACT基于关系参照理论和功能情境主义哲学取向。在干预方法上, 传统CBT聚焦内容和认知过程的有效性, 而ACT侧重功能或对认知和情绪的觉察(Hofmann & Asmundson, 2008)。因此, ACT重视提升接纳、正念、元认知和心理灵活性, 降低经验回避, 建立更为宽广、灵活、有效的应对方式, 而不仅仅是针对症状的认知和内容进行反驳(Bond et al., 2011; Hayes et al., 2011)。那么, 综合分析, 相较之传统CBT, ACT所强调的机制是否确实具有特异质呢?
其三, 这种机制在网络环境中是否能得到迁移?在影响心理治疗效果的所有因素中, 当事人与咨询师所形成的咨询同盟被认为是最大的影响因素, 咨询技术特征所带来的效果量提升较小(Wampold & Imel, 2015)。随着计算机网络化技术的发展, 近年来心理疾病的网络化干预受到较多研究者的关注, 网络化的干预使咨询同盟几乎消失, 然而一些经典的干预方法在网络环境中传播, 比如网络化CBT干预, 其作用机制仍然能得以检验(任志洪 等, 2016)。而目前基于对ACT网络化干预的作用机制的检验结果存在不一致: 比如, 一项对234名大学生群体进行心理健康的网络化干预的研究结果发现, 相较之对照组, ACT干预的心理灵活性的提升与心理健康水平提升有较强关联(Levin, Hayes, Pistorello, & Seeley, 2016), 针对抑郁的ACT网络化干预也支持心理灵活性的改变与症状改变的相关性(Lappalainen, Langrial, Oinas-Kukkonen, Tolvanen, & Lappalainen, 2015); 但也有研究发现网络化ACT干预相较之等待组, 尽管对抑郁和焦虑症状有显著的改善, 但当事人的心理灵活性并没有显著改变(Levin, Pistorello, Seeley, & Hayes, 2014)。因而, 有必要系统检验ACT所强调的作用机制在网络环境中是否能得到迁移。
1.4 本研究的目的
近年来, 元分析和结构方程结合所发展的元分析结构方程模型(Meta-analytic Structural Equation Model, MASEM) (Cheung, 2015), 使系统考察心理治疗作用机制成为可能。相较之原始单一的RCT研究, 通过两阶段MASEM汇聚多样本, 可以综合样本量, 提升模型统计力, 获得更稳定的模型估计(Montazemi & Qahri-Saremi, 2015)。
鉴于目前对ACT的作用机制缺乏系统检验, 其机制是否有区别于传统CBT的特异性, 以及在网络化干预环境的可迁移性等问题, 还未明确。本研究主要使用MASEM考察ACT的三方面作用机制:(1)检验心理灵活性及6大核心机制在ACT治疗中的中介作用; (2)考察相较之传统CBT, ACT所强调的机制是否具有特异性; (3)ACT的作用机制的可迁移性, 特别是在网络化干预中是否仍然存在。
2 研究方法
2.1 文献检索
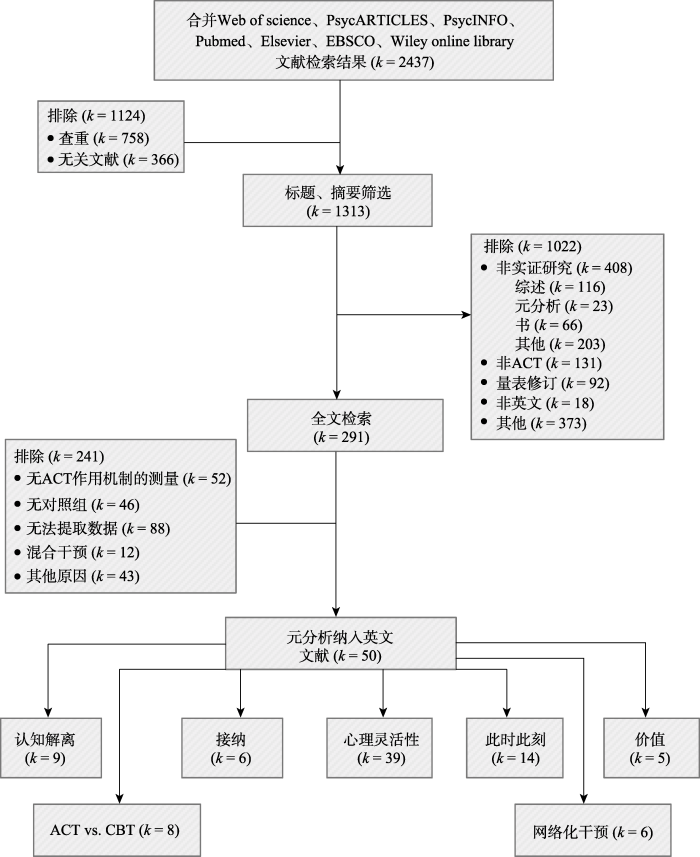
在Web of Science、PsycARTICLES、PsycINFO、PubMed、Elsevier、EBSCO、Wiley online library等数据库, 检索已经发表的英文文献。将检索关键词分为: 接纳承诺疗法(Acceptance and Commitment Therapy, ACT); 与其对应的心理机制(acceptance、cognitive defusion、self-as-context、committed action、contact with the present moment、values、psychological flexibility)进行配对组合检索。首次文献检索时间2016年10月, 2017年11月二次更新。文献由第二作者筛选, 第三作者核对, 有异议文献与第一作者协商一致解决。详细过程见图1。
图1
2.2 纳入与排除标准
文献纳入与排除标准为, 纳入: 1)成年人样本(年龄 > 18岁), 2)随机对照试验(RCT)或是准试验设计, 测量ACT干预前后变量的变化, 3)对心理健康(临床或非临床)结果前后测量改变进行定量评估, 4)对中介变量进行前后测定量评估。排除: 1)混合干预方式, 即除了ACT还包含其他干预手段, 或含有接纳成分而非完整的ACT治疗(Wicksell, Ahlqvist, Bring, Melin, & Olsson, 2008)或含接纳的行为治疗(Eustis, Hayes-Skelton, Roemer, & Orsillo, 2016; Millstein, Orsillo, Hayes-Skelton, & Roemer, 2015), 2)药物治疗对照组(Luciano et al., 2014)。
数据摘取分两类:一类是描述研究特征的基础数据, 我们采用第二作者摘取, 第三作者核对的形式; 另一类是真正纳入统计分析的核心数据, 我们采用第二作者和第三作者分别编码, 求得评分者一致性信度kappa系数为0.89, 根据在0.75及以上被认为一致性非常好的判别标准(Orwin, 1994), 说明本研究编码具有较高的一致性。最后, 与第一作者协商一致后确定最终编码。
2.3 中介检验:两阶段结构方程元分析
中介效应检验采用MASEM进行分析。Cheung (2015)提出两阶段结构方程模型(Two-Stage Structural Equation Modeling, TSSEM), 采用极大似然估计, 使标准误估计更加精确。使用R语言(Ver.3.5.2)中的metaSEM包(Ver.1.2.0)进行TSSEM分析(Cheung, 2015)。具体来说:
2.3.1 考察模型因素的测量不变性(第一阶段分析)
为了减少原始研究汇聚数据, 潜在的人为因素对结构方程参数估计的影响, 根据(Montazemi & Qahri-Saremi, 2015; Schmidt & Hunter, 2015)建议, 本研究中可能有5个人为因素影响元分析检验理论假设, 处理方法分别如下:
(1)数据的独立性。数据的非独立性违反了元分析假设(Schmidt & Hunter, 2015)。因此, 我们使用以下方法, 以保证两阶段随机效应MASEM分析数据的独立性。当一篇研究测量了多个结果时, 我们借鉴前人的系统选择方法(Gu et al., 2015): 优先选择心理病理的整体测量, 其次选择抑郁和焦虑测量结果; 同时包含他评与自评的测量结果的研究, 优先选取临床咨询师评价(Forman et al., 2007);同时测量了焦虑与抑郁的研究, 选择与样本量匹配的结果; 若是样本量不匹配, 则根据被试基线的抑郁与焦虑水平, 选取水平更高的结果; 既没有测量抑郁也没有测量焦虑的研究, 选取压力作为心理健康结果, 如果也没有压力则选择消极影响; 最后, 如果一个结果变量有两个或是多个测量工具, 则选择有更强测量学特征的结果。相对的, 若是没有包含心理健康结果的文献, 不纳入TSSEM分析。虽然可能在一项研究中计算多结果测量的均值, 但无法直接获得每项研究平均相关系数的方差, 因而, 每项研究仅提取一个心理健康结果指标较为适宜。
(2)编码过程。本研究的主要目的并非关注ACT对心理疾病治疗的效果量, 而旨在着重考察其作用机制。因而, 为了使用TSSEM考察ACT的作用机制, 从每一篇文章中提取X (ACT vs. 对照组), M变量(中介变量)在干预前后的改变以及Y变量(结果变量)干预前后的改变之间的两两相关系数, 并且提取每项研究的样本量。如果研究并没有提供明确的相关系数, 则利用均值、标准差、t值、F值和效果量(d或g值)计算相关系数(Lipsey & Wilson, 2001; Morris, 2008)。
(3)评价潜在的数据缺失影响。在元分析中, 可能存在潜在的“文件抽屉问题” (file drawer problem), 即效果不显著的论文相比效果显著的论文, 更不易被发表, 导致出版偏差(Higgins & Thompson, 2002)。我们先使用Begg and Mazumdar rank correlation和Egger’s regression intercept评估可能的出版偏差, 若存在偏差, 进而使用失安全系数(fail-safe Number, Nfs)检验可能的出版偏差对效果量的影响(Rothstein, Sutton, & Borenstein, 2005)。失安全系数是指让现有结论变得不显著的研究个数的最小值, Nfs越大, 偏倚的可能性越小; 当Nfs小于5k + 10 (k为原始研究的数目)时, 发表偏倚应引起警惕(Rothstein et al., 2005)。本研究中, 多数的Nfs值都较大(仅ACT vs. CBT的c路径可能存在出版偏差), 整体上说, 本研究结果具有较强的稳健性。
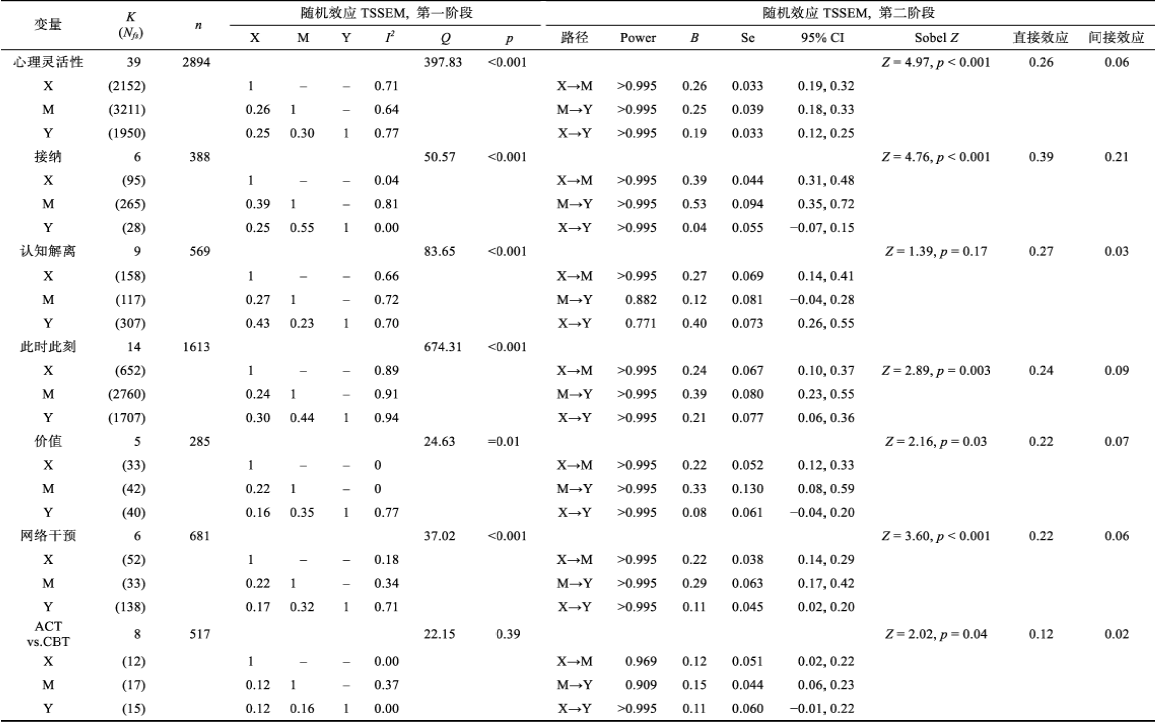
(4)检验Type II错误。统计力是统计检验中的一个重要成分, 即零假设事实不成立, 那么在多大程度上, 统计结果拒绝零假设。为了评价Type II错误的风险, 我们基于各自合并的样本量, 根据所假设检验的中介变量的合并相关系数, 使用G*Power3.1计算其统计力(Faul, Erdfelder, Lang, & Buchner, 2007)。统计力分析结果显示(表1), 除认知解离A→C的统计为0.771, 其他所有参数都大于0.8这一被广泛接受的统计力阈值。因此, 可以确信, MASEM分析的所有模型均具有足够的统计检验力以拒绝事实不成立的零假设(Cohen, 1988; Montazemi & Qahri-Saremi, 2015)。
(5) MASEM分析中原始研究异质性问题。在MASEM分析中可以使用固定效应模型(fixed-effects model)和随机效应模型(random-effects model) (Cheung, 2014)。根据Cheung和Chan (2005)的推荐, 鉴于样本、研究设计和效果量在不同研究间存在差异, 在MASEM分析中优先使用随机效应模型, 如果统计结果证明效果量是同质的, 则在第二步分析中使用固定效应模型。使用Q值和I2考察模型的异质性及其大小:Q < 0.05, 表示研究之间是异质的; I2 > 50%则为高异质性, 25%~50%为中等异质性, < 25%为低等异质性(Higgins & Thompson, 2002)。分析结果如表1所示。
2.3.2 评价SEM模型(第二阶段分析)
根据Cheung (2015)所提示的两阶段随机效应MASEM分析的步骤, 第二阶段分析是使用元分析对原始研究进行效果量合并, 结合SEM技术进行参数估计。具体来说, 因在现实中, 并非所有原始研究中涉及的变量都是同时测量的, 因此我们使用加权矩阵, 渐近协方差矩阵(asymptotic covariance matrix), 以校正合并相关系数中的异构性和每个相关矩阵中样本量的不同(Viswesvaran & Ones, 1995)。使用合并矩阵的非标准化回归系数和标准误进行Sobel检验, 以考察中介模型间接路径的显著性水平(Gu et al., 2015)。
3 结果
3.1 纳入文献基本描述
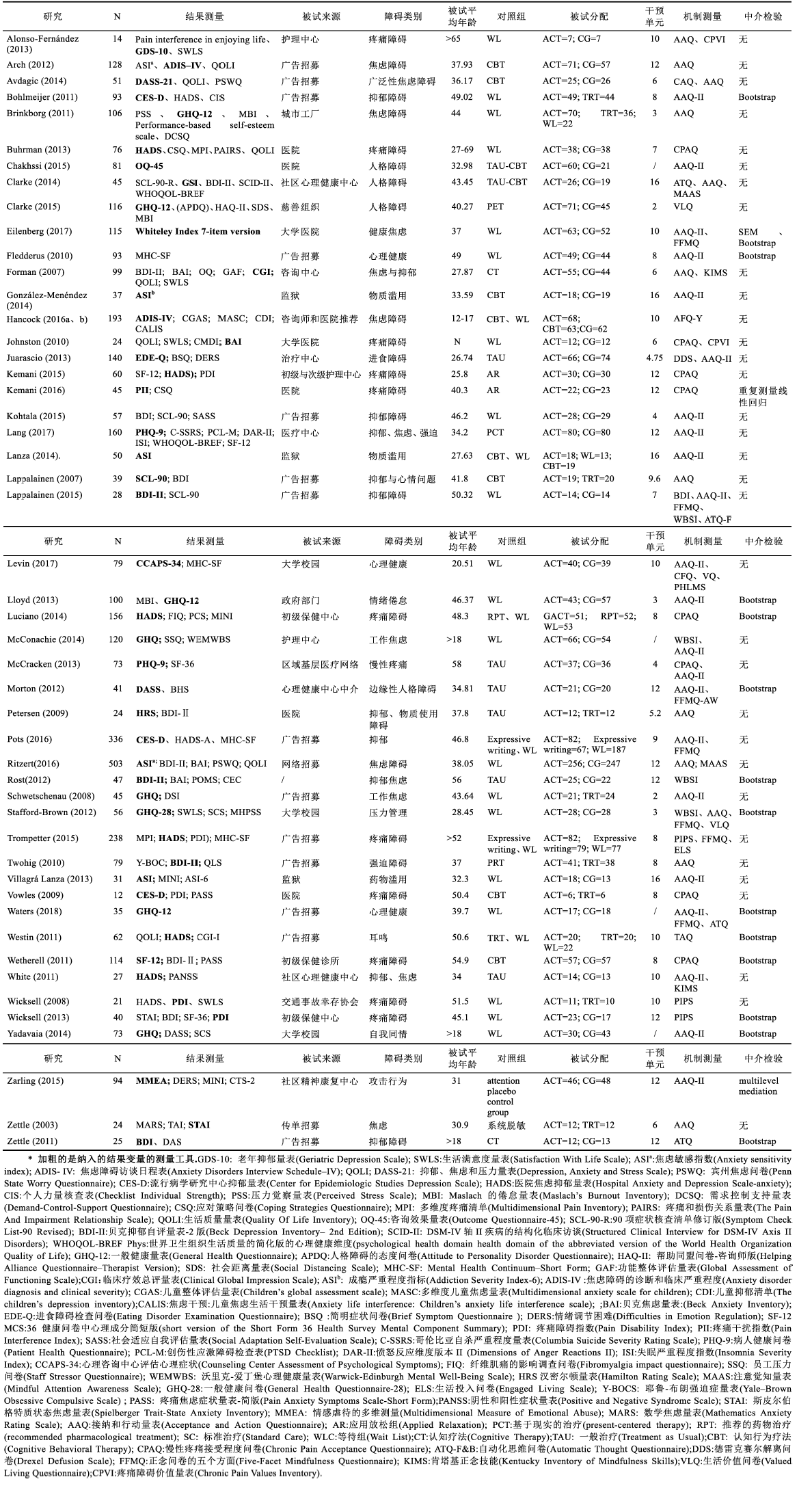
本研究最终纳入元分析文献50篇1(1纳入的元分析文献及特征编码, 请见电子版的附表。), 其中RCT研究44篇, 涉及疼痛障碍、人格障碍、抑郁、焦虑、物质滥用等多种心理问题, 甚至包括正常群体的职业倦怠等(详见电子版附录表1)。研究ACT的核心机制心理灵活性的文献最多(k = 39), 其次是此时此刻(k = 14)、接纳(k = 6)、认知解离(k = 9)和价值(k = 5), 因以已为景(Yadavaia, Hayes, & Vilardaga, 2014)和承诺行动(Avdagic, Morrissey, & Boschen, 2014)都仅纳入1篇文献, 未进行后续的MASEM分析。虽然有14篇对ACT假设的机制进行多中介变量测量(大于1项), 但并没有同时测量ACT六大作用机制的文献。纳入的文献中, 相对疗效主要以传统CBT作为对照组(k = 8); 有6项RCT考察了ACT基于网络传播的作用机制。
大多数研究测量了ACT假设的机制变量但并没有在统计上进行中介效应检验(k = 33), 仅有少数研究(k = 16)使用推荐的Bootstrap法进行中介检验(Preacher & Hayes, 2008), 个别研究仍使用传统的回归逐步检验法(Kemani, Hesser, Olsson, Lekander, & Wicksell, 2016)。当然, 也有些研究采用更为复杂的中介检验方法, 比如多水平(HLM)中介模型(Rost, Wilson, Buchanan, Hildebrandt, & Mutch, 2012; Zarling, Lawrence, & Marchman, 2015)和结构方程模型(Eilenberg, Hoffmann, Jensen, & Frostholm, 2017)。虽然在小样本分析上, HLM有优势, 但应该注意到HLM是基于正常分布假设, 而Bootstrap法在非正态分布中更具优势(Swain, Hancock, Hainsworth, & Bowman, 2015)。
实验设计上, 较少研究考虑机制变量的时序作用, 仅有8篇进行了多点测量, 但大部分多点测量使用的是前测、后测和追踪测量(Luciano et al., 2014; Stafford-Brown & Pakenham, 2012; Wetherell et al., 2011; Yadavaia et al., 2014), 追踪是在治疗结束后, 并非在有效治疗阶段; 少部分是在治疗期间测量机制变量(Lloyd, Bond, & Flaxman, 2013; Westin et al., 2011), 甚至对机制在治疗间进行多次测量(Rost et al., 2012), 但仅有极少部分在每次治疗单元都进行机制和效果测量(Kemani et al., 2016)。
3.2 ACT作用机制检验
3.2.1 心理灵活性
心理灵活性作为6大ACT作用机制的统称, 纳入研究39项, 样本量2894, 其测量主要使用接纳和行动问卷(Acceptance and Action Questionnaire, AAQ; 例如, Arch et al., 2012)、接纳和行动问卷II (Acceptance and Action Questionnaire - II, AAQ-II; 例如, Levin, Haeger, Pierce, & Twohig, 2017b)、疼痛心理的不灵活性量表(The Psychological Inflexibility in Pain Scale, PIPS) (Trompetter, Bohlmeijer, Veehof, & Schreurs, 2015; Wicksell et al., 2013)。在39项纳入研究中, 34项RCT和5项准实验研究, 以整体精神症状(Global Psychopathological Symptoms, k = 16)为主要测量结果的最多, 其次是抑郁水平(k = 9)。
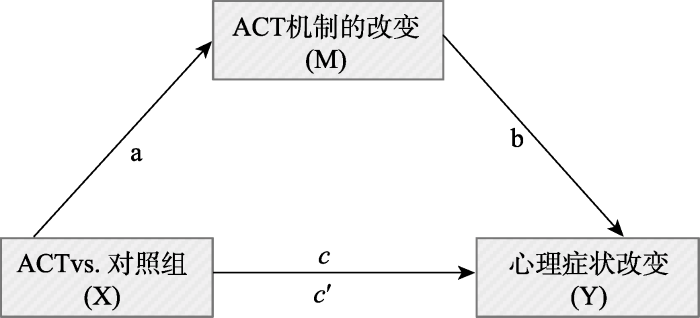
表1呈现了39项纳入研究的X, M, Y的两两相关合并系数, 三个相关系数都呈现高显著性。异质性检验发现, Q值显著(Q = 397.83, p < 0.001), 表示39项研究的相关矩阵有较大差异, 两两相关的异质性I2都大于50%, 显示较大的异质性, 适用随机效应模型。图2呈现了TSSEM分析第二阶段心理灵活性作为中介变量的模型检验路径图。虽然回归系数c' (c' = 0.19)依然显著, 但比原始c值(c = 0.25)有所下降, 为部分中介。使用X和M, M和Y的相关系数和标准误进行Sobel检验, 证明心理灵活性在ACT对心理健康的结果改变上, 起到显著的中介作用(Z = 4.97, p < 0.001)。
图2
3.2.2 接纳
纳入的研究6项, 都为RCT研究, 样本量388, 主要测量使用慢性疼痛接纳问卷(Chronic Pain Acceptance Questionnaire, CPAQ) (例如, Luciano et al., 2014)。结果测量的心理变量包括焦虑(k = 3)、抑郁(k = 2)和整体评价(k = 1)。合并效应值的三个相关系数都具有高显著性(见表1)且异质性显著(Q = 50.57, p < 0.001), 接纳具有较大程度的异质性(I2 = 0.81)。在中介的路径模型检验中, ACT的对心理健康结果的改变路径(c' = 0.04), 比直接路径(c = 0.25)有显著下降, 且c’不再显著, Sobel检验显示, 接纳在ACT与心理健康结果改变之间的中介作用显著(Z = 4.76, p < 0.001), 说明接纳在二者的关系中起到完全中介的作用。
3.2.3 认知解离
纳入的研究文献9篇(RCTs = 6, 准实验 = 3), 样本量569, 主要测量使用自动思维问卷(Automatic Thought Questionnaire, ATQ) (Clarke, Kingston, James, Bolderston, & Remington, 2014; Forman et al., 2012; Lappalainen et al., 2015; Waters, Frude, Flaxman, & Boyd, 2018; Zettle, Rains, & Hayes, 2011), 德雷塞尔解离问卷(Drexel Defusion Scale, DDS) (Juarascio et al., 2013), 白熊思维抑制量表(White Bear Thought Suppression Inventory, WBSI) (Lappalainen et al., 2015; Rost et al., 2012; Stafford-Brown & Pakenham, 2012)和青少年逃避与融合问卷(Avoidance and Fusion Questionnaire for Youth, AFQ-Y) (Levin et al., 2016)。在纳入的9篇研究中, 主要使用整体精神症状(k = 3)和抑郁(k = 3)作为结果测量。
合并效应值的三个相关系数都具有较高显著性(见表1), 异质性显著(Q = 83.65, p < 0.001)。在认知解离作为中介变量的中介模型检验中, 虽然X→Y阶段二路径系数(c' = 0.40)比阶段一系数(c = 0.43)有所下降, 但下降的值极小, 间接效应只占总效应的10%, 进一步Sobel检验显示, 认知解离在ACT与心理健康结果改变之间的中介作用不显著(Z = 1.39, p = 0.17 )。
3.2.4 此时此刻
纳入14项RCTs研究, 样本量1613, 最主要测量工具为五因素正念问卷(Five Facet Mindfulness Questionnaire, FFMQ) (例如, Eilenberg et al., 2017), 还有部分研究使用肯塔基正念技能问卷(Kentucky Inventory of Mindfulness Skills, KIMS) (Forman et al., 2007; Gumley et al., 2017; White et al., 2011), 费城正念问卷(Philadelphia Mindfulness Scale, PMS) (Levin et al., 2017b; Levin, Haeger, Pierce, & Cruz, 2017a)和正念注意觉察量表(Mindful Attention Awareness Scale, MAAS) (Clarke et al., 2014)。在纳入的研究中, 主要使用抑郁(k = 7)作为结果测量, 其次是整体精神症状(k = 6)。
合并效应值的三个相关系数都具有高显著性(见表1)且异质性显著(Q = 674.31, p < 0.001), 具有较大异质性(I2 > 89%)。在此时此刻作为中介变量的路径模型检验中, ACT对心理健康结果的改变路径(c' = 0.21), 比直接路径(c = 0.30)有显著下降, 但c'仍然保持着显著水平, Sobel检验显示, 此时此刻ACT与心理健康结果改变之间的中介作用显著(Z = 2.89, p = 0.003), 说明此时此刻在二者的关系中起到部分中介的作用。
3.2.5 价值
纳入5篇RCTs的研究文献, 样本量285, 主要测量工具为个人价值问卷(Personal Values Questionnaire, PVQ) (Levin et al., 2016), 价值问卷(Valuing Questionnaire, VQ) (Levin et al., 2017b), 慢性疼痛价值问卷(Chronic Pain Values Inventory, CPVI) (Alonso-Fernández, López-López, Losada, González, & Wetherell, 2013; Johnston, Foster, Shennan, Starkey, & Johnson, 2010), 价值生活问卷(Valued Living Questionnaire, VLQ) (Clarke, Taylor, Lancaster, & Remington, 2015; Stafford-Brown & Pakenham, 2012)。在纳入的5篇研究中, 使用整体精神症状(k = 3)和抑郁(k = 2)作为结果测量。合并效应值的三个相关系数都具有高显著性(见表1), M具有较高的异质性(I2 = 0.77), 因此仍然支持使用随机效应模型。在价值作为中介变量的路径模型检验中, ACT的对心理健康结果的改变路径(c' = 0.08), 比直接路径(c = 0.16)有显著下降, 且c'不显著, Sobel检验显示, 价值在ACT与心理健康结果改变之间的中介作用显著(Z = 2.16, p = 0.03)。
3.3 ACT相较之传统CBT作用机制的检验
以ACT作为干预组, 传统CBT作为控制组, 考察相较之传统CBT组, ACT的作用机制是否依然能被检验到。以心理灵活性作为假设的中介机制, 纳入研究文献8篇(RCTs = 7, 准实验 = 1), 样本量517, 使用整体精神症状(k = 4)和焦虑(k = 4)作为结果测量。合并效应值的三个相关系数异质性较低(I2 < 37%), 且不显著(Q = 22.15, p = 0.39)。在中介的路径模型检验中, 与传统CBT比较, ACT对心理健康结果的改变路径(c' = 0.11), 比直接路径(c = 0.12)有所下降, 但c'仍然保持着显著水平, 直接效应值为0.12, 间接效应值为0.02, Sobel检验显示, 中介作用显著(Z = 2.02, p = 0.04), 说明心理灵活性在二者的关系中起到部分中介的作用。
3.4 基于网络传播机制检验
特别考察ACT在基于网络传播的研究中, 以心理灵活性作为假设的中介机制是否依然能够得以检验。纳入6项RCT效果量(4篇文献), 样本量681, 主要使用抑郁(k = 5)作为结果测量。TSSEM的第一阶段异质性检验分析显示, 合并效应值的三个相关系数都具有高显著性(见表1), 且异质性水平显著(Q = 37.02, p < 0.001), X、M异质性水平较低(I2分别为18%和34%), 而Y异质性水平为71%。TSSEM的第二阶段分析显示, 在中介的路径模型检验中, 基于网络传播的ACT对心理健康结果的改变路径(c' = 0.11), 相较之直接路径(c = 0.17)有所下降, 但c'仍然保持着显著水平, 直接效应值为0.22, 间接效应值为0.06, Sobel检验显示, 中介作用显著(Z = 3.6, p < 0.001), 说明心理灵活性在二者的关系中起到部分中介的作用。
4 讨论
本研究采用MASEM的方法, 系统检验了ACT所假设的作用机制。其一, 在疼痛障碍、人格障碍、抑郁(障碍)、焦虑(障碍)、物质滥用、职业倦怠等不同群体, ACT所假设的心理灵活性、接纳、此时此刻、价值的中介作用都达到统计显著, 认知解离这一中介变量并不显著, 而以已为景和承诺行动因各只纳入一篇研究无法进行MASEM分析。其二, 这些机制在网络化干预中仍然得到检验, 说明ACT的治疗机制具有可迁移性。
其三, ACT在其所假设的改变机制上, 即心理灵活性及其所包含的6大成分, 较传统CBT具有优势。与以往的元分析发现较为一致(Dimidjian et al., 2016)的是ACT在其相关联的过程变量改变上, 相较之传统CBT, 具有中等后测效果量(g = 0.45)。但应看到的, 在与传统CBT的对比中, 本元分析纳入的研究多数仅测量了心理灵活性。ACT对特定机制具有更大效果量, 并不意味着治疗效果更好, 目前元分析的证据并无法得出ACT比传统CBT更有效的结论(Dimidjian et al., 2016; Hacker et al., 2016; Öst, 2008; Öst, 2014; Powers, Vörding, & Emmelkamp, 2009), 但是, 正如共同因素说所主张的“渡渡鸟效应”, 凡是有效的治疗机制都应该被奖励, 这有助于后续研究进一步厘清不同治疗方法共同的作用机制。正如ACT与以人为中心治疗的比较研究中发现的: 以人为中心疗法对ACT所提出的心理灵活性具有同等的改变效果(Lang et al., 2017)。
值得注意的是, ACT中认知解离的中介效应不显著。可能的原因是, 在纳入测量认知解离的9篇文献中, 有3篇的对照组是传统CBT或CT组(Clarke et al., 2014; Hancock & Swain, 2016; Hancock et al., 2016; Zettle et al., 2011), 而ACT与传统CBT (或CT)可能都发生了认知解离。
不少研究者认为, ACT所提出的认知解离和传统CBT的认知重建概念具有异曲同工之处(Dimidjian et al., 2016; Swain et al., 2015), 研究者推测二者可能有潜在相同的作用机制(Forman et al., 2012)。虽然传统CBT并没有明确讨论认知解离, 但有研究提供了证据, 即认知解离不仅在ACT中发生改变, 在传统CBT中同样发生(Arch et al., 2012); 而ACT疗法也同样改变了传统CBT中所强调的功能失调性思维(任志洪 等, 2016)。认知解离被定义为减少认知的字面性质, 其结果是“通常减少对个体事件的可信度或依附性”(Hayes et al., 2006), 换言之, 把负性思维看作一种行为, 从而更好地把事件与所衍生的意义分离(Larsson, Hooper, Osborne, Bennett, & McHugh, 2016)。而在传统CBT中, 这种现象也被称为元认知觉察(metacognitive awareness), 即“负性思维认知……被看作是个体经历的心理事件, 而非自我本身”(Takahashi, Muto, Tada, & Sugiyama, 2002)。这些证据表明了ACT认知解离与传统CBT认知重建的重叠性, 即降低认知的可信度。如何降低认知可信度呢? 有研究者进一步指出, 认知重建和接纳有助于降低对心理事件的抑制和心理回避, 而这过程包括聚焦、识别和打断消极思维, 这可能也是一种暴露形式(Swain et al., 2015); 而ACT的诸多练习, 比如单词游戏(单词重复、搞怪声音、慢说话、唱出思维、单词翻译), 这些暴露程序使当事人反复接触高频度的相关刺激, 直到其语言所引出的功能减弱(Assaz, Roche, Kanter, & Oshiro, 2018)。简言之, 暴露可能是认知解离与认知重建共同的作用机制。
本研究的局限: (1)本研究仅关注随机和非随机对照组研究, 而其他类型的研究, 比如个案研究, 可能可以为ACT的作用机制在治疗过程中的变化提供更为深入的理解; (2)所纳入的实证研究, 其研究对象、精神障碍或心理问题类型不尽相同, 各项实证研究的具体操作和数据收集方法具有差异。这也正是元分析一直存在的“苹果和橙子问题” (apple and orange problem); 但纳入元分析的实证研究也具有共性, 都关注ACT对精神障碍或心理问题的治疗效果, 这些共性是元分析得以进行的基础。(3)从理论假设上来说, 6个成分应是一阶因素, Hayes用心理灵活性一词作为6大机制的统称, 那么心理灵活性应该是二阶因素。所以, 可能存在更为复杂的机制模型, 比如, ACT治疗→某个ACT成分→心理灵活性→治疗效果, 或者是: ACT治疗→心理灵活性→某个ACT成分变化→治疗效果。然而, 元分析是基于已有实证研究的再分析, 而在纳入的实证研究中极少同时测量了心理灵活性及6大成分, 因此在本研究中, 我们无法检验更为复杂的ACT作用机制模型。(4) MASEM方法本身具有一定的局限性, 特别是本研究对作用机制的考察报告了Sobel经典中介检验结果, 该法近年来也受到正态分布假设和统计功效较低的诟病(MacKinnon, et al., 2007); 且应该注意到, 原始研究中其中介变量和治疗结果变量的测量方法可能存在共同测量偏差, 本研究结果可能也受其影响。
5 临床研究启示
(1)应尽可能全面测量ACT的6大核心机制。现有研究主要使用的AAQ和AAQ-II更趋向于测量全局的心理灵活性, 而对6大具体核心机制的检验较少。许多研究并没有同时测量6大作用机制, 可能是其测量工具上的不便, 不同的机制使用了不同的测量工具。因而, 最近有研究者开发同时测量ACT六大成分的测量工具(Francis, Dawson, & Golijani-Moghaddam, 2016), 虽然其信效度仍需临床研究进一步检验。
(2)现有对ACT的研究聚集于症状的改善, 后续研究应关注其对美好生活提升的影响。一些观点认为, ACT的6大机制可以分为三大模块(Villatte et al., 2016): 接纳和认知解离属于“开放”模块, 目的是降低思维、情感和感觉的有害反应; 价值和承诺行动属于“行动”模块, 侧重强化动机和增加有意义行为; 而接触当下和以已为景主要是为了促进自我觉察, 在“开放”和“行动”模块中都包含, 但并没有特意强调。就纳入本元分析的文献而言, 多数研究聚集的是“开放”模块, 而对“行动”模块的关注较少。事实上, “行动”模块具有极为重要的意义。一方面是, 接纳承诺疗法倡导者Hayes一再强调应该把该疗法的缩写“ACT” (Acceptance and Commitment Therapy)读成Act (行动), 而不是逐字母读成“A-C-T”, 以体现该疗法中“承诺行动”的重要性; 另一方面, 在积极心理学的影响下, 心理健康的双因素模型认为, 心理健康并非仅是没有心理疾病, 还应有较高的幸福感(Keyes, Shmotkin, & Ryff, 2002)。聚集于接纳和认知解离的干预机制在降低心理疾病症状上有较大效果; 而价值和承诺行动则更有助于提升幸福感水平(Villatte et al., 2016)。此外, 对很多症状来说, 特别是一些与躯体相关的心理症状, 比如疼痛障碍, 其生理和心理症状本身可能并不能彻底根除, 这就需要当事人学会与症状较长时间相处, 那么帮助当事人寻求过与自己价值一致的生活, 就显得尤为重要。
(3)研究设计上建议基于RCT多点测量, 结合瞬时评价方法。几乎所有的研究都没有满足治疗研究中介变量检验的要求。可能识别中介变量研究的最大挑战是证明中介变量的改变而导致症状的改变这一因果关系。因此, 尽管经过30多年的过程研究, 仍无法对心理治疗的改变机制有清晰、明确的实验解释(Lemmens et al., 2016)。即使是旨在考察治疗改变的因果过程研究, 欲证明因果关系也是很困难的。首先, 确定观测的最佳时间和间隔, 以捕获治疗改变的临界点, 是一件困难而微妙的事情, 特别是在治疗的变化速度和形态并没有先验信息的情况下。研究者需要在最优化研究设计、当事人负担和对数据过多测量所造成的测量假象风险等方面获得平衡(Longwell & Truax, 2005)。此外, 研究设计通常是基于治疗改变是渐进和线性的假设。然而, 各种研究表明, 改变经常是突然发生的, 而不是在治疗过程中逐渐发生(Aderka, Nickerson, Bøe, & Hofmann, 2012)。如果治疗确实是突然获益(例如“啊哈体验”), 那么抓住这一时刻可能非常困难, 更不用说评估机制变化与症状改变之间的时序关系(Lemmens et al., 2016)。然而, 随着网络化干预发展, 特别是基于手机APP干预应用的尝试(Levin et al., 2017a), 结合当事人主动报告瞬时评价的日常经验取样法(Experience Sampling Method) (Hektner, Schmidt, & Csikszentmihalyi, 2007)去捕获干预的突然获益逐渐成为可能, 这将有助于厘清改变机制。
(4)在传统中介检验法的基础上, 尽可能使用更高级、更先进的统计方法。根据Kazdin (2007)治疗中介检验的建议, 现有治疗机制检验多数采用推荐的Bootstrap法进行中介检验(Preacher & Hayes, 2008)。而一些研究者认为, 仅通过前后测(或追踪)探索治疗的改变机制是不足够的, 要考察治疗过程中介变量和结果变量的变化趋势, 应该在治疗期间对二者进行多点测量(Black & Chung, 2014)。极少ACT研究者开始在每次治疗单元都进行机制和效果测量, 并使用与多点测量相对应的纵向中介模型分析; 而已有研究大多采用混合效应回归模型, 即以时间、中介变量和结果变量为层一, 被试个体间差异为层二, 以考察随着时间变化每干预单元机制与结果变量的变化情况(Forman et al., 2012; Kemani et al., 2016)。然而, 近年来新发展的纵向中介模型分析技术(Grimm, Ram, & Estabrook, 2017), 比如潜变量增长曲线模型(Latent Growth Curve Models, LGCM)、潜变量变化分数模型(Latent Change Score Models)和多水平结构方程模型(Multilevel Structural Equation Modeling)也应值得尝试。
6 结论
本研究采用元分析结构方程模型, 通过对50篇ACT研究中介机制的检验, 得出以下结论:(1) ACT所假设的心理灵活性、接纳、此时此刻、价值的中介作用都达到统计显著; 认知解离这一中介变量并不显著; (2) ACT在所假设的机制上有其区别于传统CBT的优势; (3)这些机制在网络化干预中仍然得到检验, 说明ACT治疗的机制具有可迁移性。
附录2:元分析纳入文献
Arch, J. J., Eifert, G. H., Davies, C., Vilardaga, J. C. P., Rose, R. D., & Craske, M. G. (2012). Randomized clinical trial of cognitive behavioral therapy (CBT) versus acceptance and commitment therapy (ACT) for mixed anxiety disorders. Journal of Consulting and Clinical Psychology, 80(5), 750-765.
Avdagic, E., Morrissey, S. A., & Boschen, M. J. (2014). A randomised controlled trial of acceptance and commitment therapy and cognitive-behaviour therapy for generalised anxiety disorder. Behaviour Change, 31(2), 110-130.
Aderka, I. M., Nickerson, A., Bøe, H. J., & Hofmann, S. G. (2012). Sudden gains during psychological treatments of anxiety and depression: A meta-analysis. Journal of Consulting and Clinical Psychology, 80(1), 93-101.
Bohlmeijer, E. T., Fledderus, M., Rokx, T. A. J. J., & Pieterse, M. E. (2011). Efficacy of an early intervention based on acceptance and commitment therapy for adults with depressive symptomatology: Evaluation in a randomized controlled trial. Behaviour Research and Therapy, 49(1), 62-67.
Brinkborg, H., Michanek, J., Hesser, H., & Berglund, G. (2011). Acceptance and commitment therapy for the treatment of stress among social workers: A randomized controlled trial. Behaviour Research and Therapy, 49(6-7), 389-398.
Buhrman, M., Skoglund, A., Husell, J., Bergström, K., Gordh, T., Hursti, T., … Andersson, G. (2013). Guided internet-delivered acceptance and commitment therapy for chronic pain patients: A randomized controlled trial. Behaviour Research and Therapy, 51(6), 307-315.
Chakhssi, F., Janssen, W., Pol, S. M., van Dreumel, M., & Westerhof, G. J. (2015). Acceptance and commitment therapy group‐treatment for non‐responsive patients with personality disorders: An exploratory study. Personality and Mental Health, 9(4), 345-356.
Clarke, S., Kingston, J., James, K., Bolderston, H., & Remington, B. (2014). Acceptance and commitment therapy group for treatment-resistant participants: A randomized controlled trial. Journal of Contextual Behavioral Science, 3(3), 179-188.
Clarke, S., Taylor, G., Lancaster, J., & Remington, B. (2015). Acceptance and commitment therapy-based self-management versus psychoeducation training for staff caring for clients with a personality disorder: A randomized controlled trial. Journal of Personality Disorders, 29(2), 163-176.
Eilenberg, T., Hoffmann, D., Jensen, J. S., & Frostholm, L. (2017). Intervening variables in group-based acceptance & commitment therapy for severe health anxiety. Behaviour Research and Therapy, 92, 24-31.
Fledderus, M., Bohlmeijer, E. T., Smit, F., & Westerhof, G. J. (2010). Mental health promotion as a new goal in public mental health care: A randomized controlled trial of an intervention enhancing psychological flexibility. American Journal of Public Health, 100(12), 2372-2378.
Forman, E. M., Herbert, J. D., Moitra, E., Yeomans, P. D., & Geller, P. A. (2007). A randomized controlled effectiveness trial of acceptance and commitment therapy and cognitive therapy for anxiety and depression. Behavior Modification, 31(6), 772-799.
González-Menéndez, A., Fernández, P., Rodríguez, F., & Villagrá, P. (2014). Long-term outcomes of acceptance and commitment therapy in drug-dependent female inmates: A randomized controlled trial. International Journal of Clinical and Health Psychology, 14(1), 18-27.
Hancock, K., & Swain, J. (2016). Long term follow up in children with anxiety disorders treated with acceptance and commitment therapy or cognitive behavioral therapy: Outcomes and predictors. Journal of Child and Adolescent Behavior, 4(5), 317-329.
Hancock, K. M., Swain, J., Hainsworth, C. J., Dixon, A. L., Koo, S., & Munro, K. (2016). Acceptance and commitment therapy versus cognitive behavior therapy for children with anxiety: Outcomes of a randomized controlled trial. Journal of Clinical Child and Adolescent Psychology, 47(2), 296-311.
Johnston, M., Foster, M., Shennan, J., Starkey, N. J., & Johnson, A. (2010). The effectiveness of an acceptance and commitment therapy self-help intervention for chronic pain. Clinical Journal of Pain, 26(5), 393-402.
Juarascio, A., Shaw, J., Forman, E., Timko, C. A., Herbert, J., Butryn, M., et al. (2013). Acceptance and commitment therapy as a novel treatment for eating disorders: An initial test of efficacy and mediation. Behavior Modification, 37(4), 459-489.
Kemani, M. K., Hesser, H., Olsson, G. L., Lekander, M., & Wicksell, R. K. (2016). Processes of change in acceptance and commitment therapy and applied relaxation for long-standing pain. European Journal of Pain, 20(4), 521-531.
Kohtala, A., Lappalainen, R., Savonen, L., Timo, E., Tolvanen, A. (2015). A four-session acceptance and commitment therapy based intervention for depressive symptoms delivered by masters degree level psychology students: A Preliminary Study. Behavioural and Cognitive Psychotherapy, 43(3), 360-373.
Kemani, M. K., Olsson, G. L., Lekander, M., Hesser, H., Andersson, E., & Wicksell, R. K. (2015). Efficacy and cost-effectiveness of acceptance and commitment therapy and applied relaxation for longstanding pain: A randomized controlled trial. Clinical Journal of Pain, 31(11), 1004-1016.
Lloyd, J., Bond, F. W., & Flaxman, P. E. (2013). The value of psychological flexibility: Examining psychological mechanisms underpinning a cognitive behavioural therapy intervention for burnout. Work and Stress, 27(2), 181-199.
Luciano, J. V., Guallar, J. A., Aguado, J., Lopez-del-Hoyo, Y., Olivan, B., Magallon, R., … Garcia-Campayo, J. (2014). Effectiveness of group acceptance and commitment therapy for fibromyalgia: A 6-month randomized controlled trial (EFFIGACT study). PAIN®, 155(4), 693-702.
Lanza, P. V., García, P. F., Lamelas, F. R., & González-Menéndez, A. (2014). Acceptance and commitment therapy versus cognitive behavioral therapy in the treatment of substance use disorder with incarcerated women. Journal of Clinical Psychology, 70(7), 644-657.
Levin, M. E., Haeger, J. A., Pierce, B. G., & Twohig, M. P. (2017). Web-based acceptance and commitment therapy for mental health problems in college students: A randomized controlled trial. Behavior Modification, 41(1), 141-162.
Lappalainen, P., Langrial, S., Oinas-Kukkonen, H., Tolvanen, A., & Lappalainen, R. (2015). Web-based acceptance and commitment therapy for depressive symptoms with minimal support: A randomized controlled trial. Behavior Modification, 39(6), 805-834.
Lappalainen, R., Lehtonen, T., Skarp, E., Taubert, E., Ojanen, M., & Hayes, S. C. (2007). The impact of CBT and ACT models using psychology trainee therapists: A preliminary controlled effectiveness trial. Behavior Modification, 31(4), 488-511.
Lang, A. J., Schnurr, P. P., Jain, S., He, F., Walser, R. D., Bolton, E., ... Strauss, J. (2017). Randomized controlled trial of acceptance and commitment therapy for distress and Impairment in OEF/OIF/OND veterans. Psychological Trauma: Theory, Research, Practice, and Policy, 9(S1), 74-84.
McConachie, D. A. J., McKenzie, K., Morris, P. G., & Walley, R. M. (2014). Acceptance and mindfulness-based stress management for support staff caring for individuals with intellectual disabilities. Research in Developmental Disabilities, 35(6), 1216-1227.
Morton, J., Snowdon, S., Gopold, M., & Guymer, E. (2012). Acceptance and commitment therapy group treatment for symptoms of borderline personality disorder: A public sector pilot study. Cognitive and Behavioral Practice, 19(4), 527-544.
McCracken, L. M., Sato, A., & Taylor, G. J. (2013). A trial of a brief group-based form of acceptance and commitment therapy (ACT) for chronic pain in general practice: Pilot outcome and process results. The Journal of Pain, 14(11), 1398-1406.
Pots, W. T. M., Fledderus, M., Meulenbeek, P. A. M., Klooster, P. M. ten, Schreurs, K. M. G., & Bohlmeijer, E. T. (2016). Acceptance and commitment therapy as a web-based intervention for depressive symptoms: Randomised controlled trial. The British Journal of Psychiatry, 208(1), 69-77.
Petersen, C. L., & Zettle, R. D. (2009). Treating inpatients with comorbid depression and alcohol use disorders: A comparison of acceptance and commitment therapy versus treatment as usual. The Psychological Record, 59(4), 521-536.
Ritzert, T. R., Forsyth, J. P., Sheppard, S. C., Boswell, J. F., Berghoff, C. R., & Eifert, G. H. (2016). Evaluating the effectiveness of ACT for anxiety disorders in a self-help context: Outcomes from a randomized wait-list controlled trial. Behavior Therapy, 47(4), 444-459.
Rost, A. D., Wilson, K., Buchanan, E., Hildebrandt, M. J., & Mutch, D. (2012). Improving psychological adjustment among late-stage ovarian cancer patient: Examining the role of avoidance in treatment. Cognitive and Behavioral Practice, 19(4), 508-517.
Schwetschenau, M. H. (2008). The effectiveness of an acceptance and commitment intervention for work stress (Unpublished doctorial dissertation). Bowling Green State University.
Stafford-Brown, J., & Pakenham, K. I. (2012). The effectiveness of an act informed intervention for managing stress and improving therapist qualities in clinical psychology trainees. Journal of Clinical Psychology, 68(6), 592-513.
Trompetter, H. R., Bohlmeijer, E. T., Veehof, M. M., & Schreurs, K. M. G. (2015). Internet-based guided self-help intervention for chronic pain based on acceptance and commitment therapy: A randomized controlled trial. Journal of Behavioral Medicine, 38(1), 66-80.
Twohig, M. P., & Crosby, J. M. (2010). Acceptance and commitment therapy as a treatment for problematic internet pornography viewing. Behavior Therapy, 41(3), 285-295.
Villagrá, L. P., & González, M. A. (2013). Acceptance and commitment therapy for drug abuse in incarcerated women. Psicothema, 25(3), 307-312.
Vowles, K. E., Wetherell, J. L., & Sorrell, J. T. (2009). Targeting acceptance, mindfulness, and values-based action in chronic pain: Findings of two preliminary trials of an outpatient group-based intervention. Cognitive and Behavioral Practice, 16(1), 49-58.
Wicksell, R. K., Ahlqvist, J., Bring, A., Melin, L., & Olsson, G. L. (2008). Can exposure and acceptance strategies improve functioning and life satisfaction in people with chronic pain and whiplash-associated disorders (WAD)? A randomized controlled trial. Cognitive Behaviour Therapy, 37(3), 169-182.
Wetherell, J. L., Afari, N., Rutledge, T., Sorrell, J. T., Stoddard, J. A., Petkus, A. J., … Atkinson, J. (2011). A randomized, controlled trial of acceptance and commitment therapy and cognitive-behavioral therapy for chronic pain. Pain, 152(9), 2098-2107.
Waters, C. S., Frude, N., Flaxman, P. E., & Boyd, J. (2018). Acceptance and commitment therapy (ACT) for clinically distressed health care workers: Waitlist-controlled evaluation of an ACT workshop in a routine practice setting. British Journal of Clinical Psychology, 57(4), 82-98.
White, R., Gumley, A., McTaggart, J., Rattrie, L., McConville, D., Cleare, S., & Mitchell, G. (2011). A feasibility study of acceptance and commitment therapy for emotional dysfunction following psychosis. Behaviour Research and Therapy, 49(12), 901-907.
Yadavaia, J. E., Hayes, S. C., & Vilardaga, R. (2014). Using acceptance and commitment therapy to increase self-compassion: A randomized controlled trial. Journal of Contextual Behavioral Science, 3(4), 248-257.
Wicksell, R. K., Kemani, M., Jensen, K., Kosek, E., Kadetoff, D., Sorjonen, K., … Olsson, G. L. (2013). Acceptance and commitment therapy for fibromyalgia: A randomized controlled trial. European Journal of Pain, 17(4), 599-611.
Westin, V. Z., Schulin, M., Hesser, H., Karlsson, M., Noe, R. Z., Olofsson, U., … Andersson, G. (2011). Acceptance and commitment therapy versus tinnitus retraining therapy in the treatment of tinnitus: A randomised controlled trial. Behaviour Research and Therapy, 49(11), 737-747.
Zettle, R. D. (2003). Acceptance and commitment therapy (ACT) vs. systematic desensitization in treatment of mathematics anxiety. Psychological Record, 53(2), 197-215.
Zarling, A., Lawrence, E., & Marchman, J. (2015). A randomized controlled trial of acceptance and commitment therapy for aggressive behavior. Journal of Consulting and Clinical Psychology, 83(1), 199-212.
Zettle, R. D., Rains, J. C., & Hayes, S. C. (2011). Processes of change in acceptance and commitment therapy and cognitive therapy for depression: A mediation reanalysis of Zettle and Rains. Behavior Modification, 35(3), 265-283.
参考文献
Sudden gains during psychological treatments of anxiety and depression: A meta-analysis
DOI:10.1037/a0026455
URL
PMID:22122290
[本文引用: 1]

The present study quantitatively reviewed the literature on sudden gains in psychological treatments for anxiety and depression. The authors examined the short- and long-term effects of sudden gains on treatment outcome as well as moderators of these effects.The authors conducted a literature search using PubMed, PsycINFO, the Cochrane Library, and manual searches. The meta-analysis was based on 16 studies and included 1,104 participants receiving psychological treatment for major depressive disorder or an anxiety disorder.Effect size estimates suggest that sudden gains had a moderate effect on primary outcome measures at posttreatment (Hedges's g = 0.62) and follow-up (Hedges's g = 0.56). These effect sizes were robust and unrelated to publication year or number of treatment sessions. The effect size of sudden gains in cognitive-behavioral therapy was higher (Hedges's g = 0.75) than in other treatments (Hedges's g = 0.23).These results suggest that sudden gains are associated with short-term and long-term improvements in depression and anxiety, especially in cognitive-behavioral therapy.
Acceptance and commitment therapy and selective optimization with compensation for institutionalized older people with chronic pain: A pilot study
DOI:10.1111/pme.12885
URL
PMID:26304771
[本文引用: 1]
ABSTRACT Objective Recent studies support the efficacy of Acceptance and Commitment Therapy (ACT) with people with chronic pain. In addition, Selective Optimization with Compensation strategies (SOC) can help the elderly with chronic pain to accept their chronic condition and increase functional autonomy. Our aim was to analyze the efficacy of an ACT treatment program combined with training in SOC strategies for elderly people with chronic pain living in nursing homes. Methods 101 participants (mean age = 82.26; SD = 10.00; 78.6% female) were randomized to the intervention condition (ACT-SOC) or to a minimal support group (MS). Complete data are available for 53 participants (ACT-SOC: n = 27; MS: n = 26). Assessments of functional performance, pain intensity, pain acceptance, SOC strategies, emotional well being and catastrophizing beliefs were done preintervention and postintervention. Results Significant time by intervention changes (P = 0.05) were found in acceptance, pain related anxiety, compensation strategies, and pain interference in walking ability. Simple effects changes were found in acceptance (P = 0.01), selection strategies (P = 0.05), catastrophizing beliefs (P = 0.03), depressive symptoms (P = 0.05), pain anxiety (P = 0.01) and pain interference in mood and walking ability (P = 0.03) in the ACT-SOC group. No significant changes were found in the MS group. Conclusions These results suggest that an ACT intervention combined with training in SOC strategies could help older people with pain to improve their emotional well being and their functional capability.
Mechanisms of action in mindfulness-based cognitive therapy (MBCT) and mindfulness-based stress reduction (MBSR) in people with physical and/or psychological conditions: A systematic review
DOI:10.1016/j.cpr.2017.04.008 URL [本文引用: 1]
Randomized clinical trial of cognitive behavioral therapy (CBT) versus acceptance and commitment therapy (ACT) for mixed anxiety disorders
DOI:10.1037/a0028310
URL
PMID:22563639
[本文引用: 2]
Randomized comparisons of acceptance-based treatments with traditional cognitive behavioral therapy (CBT) for anxiety disorders are lacking. To address this gap, we compared acceptance and commitment therapy (ACT) to CBT for heterogeneous anxiety disorders.One hundred twenty-eight individuals (52% female, mean age = 38, 33% minority) with 1 or more DSM-IV anxiety disorders began treatment following randomization to CBT or ACT; both treatments included behavioral exposure. Assessments at pre-treatment, post-treatment, and 6- and 12-month follow-up measured anxiety-specific (principal disorder Clinical Severity Ratings [CSRs], Anxiety Sensitivity Index, Penn State Worry Questionnaire, Fear Questionnaire avoidance) and non-anxiety-specific (Quality of Life Index [QOLI], Acceptance and Action Questionnaire-16 [AAQ]) outcomes. Treatment adherence, therapist competency ratings, treatment credibility, and co-occurring mood and anxiety disorders were investigated.CBT and ACT improved similarly across all outcomes from pre- to post-treatment. During follow-up, ACT showed steeper linear CSR improvements than CBT (p < .05, d = 1.26), and at 12-month follow-up, ACT showed lower CSRs than CBT among completers (p < .05, d = 1.10). At 12-month follow-up, ACT reported higher AAQ than CBT (p = .08, d = 0.42; completers: p < .05, d = 0.56), whereas CBT reported higher QOLI than ACT (p < .05, d = 0.42). Attrition and comorbidity improvements were similar; ACT used more non-study psychotherapy at 6-month follow-up. Therapist adherence and competency were good; treatment credibility was higher in CBT.Overall improvement was similar between ACT and CBT, indicating that ACT is a highly viable treatment for anxiety disorders.
Cognitive defusion in acceptance and commitment therapy: What are the basic processes of change
DOI:10.1007/s40732-017-0254-z [本文引用: 1]
A meta-analysis of the efficacy of acceptance and commitment therapy for clinically relevant mental and physical health problems
DOI:10.1159/000365764
URL
PMID:25547522
[本文引用: 1]
Abstract BACKGROUND: The current study presents the results of a meta-analysis of 39 randomized controlled trials on the efficacy of acceptance and commitment therapy (ACT), including 1,821 patients with mental disorders or somatic health problems. METHODS: We searched PsycINFO, MEDLINE and the Cochrane Central Register of Controlled Trials. Information provided by the ACBS (Association of Contextual Behavioral Science) community was also included. Statistical calculations were conducted using Comprehensive Meta-Analysis software. Study quality was rated using a methodology rating form. RESULTS: ACT outperformed control conditions (Hedges' g = 0.57) at posttreatment and follow-up assessments in completer and intent-to-treat analyses for primary outcomes. ACT was superior to waitlist (Hedges' g = 0.82), to psychological placebo (Hedges' g = 0.51) and to treatment as usual (TAU) (we defined TAU as the standard treatment as usual; Hedges' g = 0.64). ACT was also superior on secondary outcomes (Hedges' g = 0.30), life satisfaction/quality measures (Hedges' g = 0.37) and process measures (Hedges' g = 0. 56) compared to control conditions. The comparison between ACT and established treatments (cognitive behavioral therapy) did not reveal any significant differences between these treatments (p = 0.140). CONCLUSIONS: Our findings indicate that ACT is more effective than treatment as usual or placebo and that ACT may be as effective in treating anxiety disorders, depression, addiction, and somatic health problems as established psychological interventions. More research that focuses on quality of life and processes of change is needed to understand the added value of ACT and its transdiagnostic nature. 2014 S. Karger AG, Basel.
A randomised controlled trial of acceptance and commitment therapy and cognitive-behaviour therapy for generalised anxiety disorder
DOI:10.1017/bec.2014.5 URL [本文引用: 1]
The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations
DOI:10.1037/0022-3514.51.6.1173 URL [本文引用: 1]
Cognitive therapy: Past, present, and future
DOI:10.1037/0022-006X.61.2.194
URL
PMID:8473571
[本文引用: 1]
Proponents of cognitive therapy have striven to establish this approach as a mature system of psychotherapy for over 3 decades. The theoretical formulations have been enriched by clinical extrapolations from the neopsychoanalysts and experimental findings from cognitive psychology. The therapeutic strategies and techniques have been refined as a result of interaction with therapy, which also influenced the emphasis on empirical testing of the theoretical formulations and the therapeutic applications. Outcome trials have demonstrated efficacy in a number of common disorders. New emphasis on the crucial importance of specific formulations (especially dysfunctional beliefs) has provided important clues to the treatment of a large number of other disorders. I conclude that cognitive therapy has fulfilled the criteria of a system of psychotherapy by providing a coherent, testable theory of personality, psychopathology, and therapeutic change; a teachable, testable set of therapeutic principles, strategies, and techniques that articulate with the theory; and a body of clinical and empirical data that support the theory and the efficacy of the theory.
Mechanisms of change in adolescent substance use treatment: How does treatment work?
DOI:10.1080/08897077.2014.925029
URL
PMID:4257904
[本文引用: 1]
ABSTRACT. Background: Adolescent substance use treatment outcome research generally shows small to moderate effects in reducing substance use, with no specific “brand” of treatment emerging as clearly superior to any other, and treatment gains that fade over time. The relatively weak and temporary effects of treatment call for improving the potency and durability of intervention effects. In response to this call, this critical narrative review summarizes research on mechanisms of change for both adults and adolescents in substance use treatment, with a particular focus on reviewing what is known regarding “how” adolescent substance use treatment works. Methods: A comprehensive review of the adolescent (aged 11–18) substance use treatment literature was conducted to identify empirical studies that examined mediators of intervention effects. Relevant databases (e.g., PsychINFO, MEDLINE) were searched using key words (e.g., “mediator”), and relevant articles from reference sections of identified studies and review papers were considered. Results: Studies of mechanisms of psychotherapy change are rare in the adult, and particularly adolescent, substance use treatment outcome literature. The 4 adolescent studies that examined substance use treatment mechanisms found that positive social support, motivation to abstain, and positive parenting behaviors mediated treatment effects. To date, research has not supported therapy-specific mechanisms of change, finding instead that “common” processes of change largely account for improvements in outcome across distinct “brands” of treatment. Conclusions: The lack of empirical support for treatment-specific mechanisms of change may be due to the need for greater precision in defining and measuring treatment-specific causal chains. Future directions include neuroscience approaches to examining changes in brain functioning that are associated with treatment response and recovery and examining mechanisms in adaptive treatment designs, which can accommodate individual differences in targets for intervention and response to treatment.
Acceptance and commitment therapy for anxiety and OCD spectrum disorders: An empirical review
DOI:10.1016/j.janxdis.2014.06.008
URL
PMID:25041735
[本文引用: 1]
A fair amount of research exists on acceptance and commitment therapy (ACT) as a model and a treatment for anxiety disorders and OCD spectrum disorders; this paper offers a quantitative account of this research. A meta-analysis is presented examining the relationship between psychological flexibility, measured by versions of the Acceptance and Action Questionnaire (AAQ and AAQ-II) and measures of anxiety. Meta-analytic results showed positive and significant relationships between the AAQ and general measures of anxiety as well as disorder specific measures. Additionally, all outcome data to date on ACT for anxiety and OCD spectrum disorders are reviewed, as are data on mediation and moderation within ACT. Preliminary meta-analytic results show that ACT is equally effective as manualized treatments such as cognitive behavioral therapy. Future directions and limitations of the research are discussed.
Preliminary psychometric properties of the Acceptance and Action Questionnaire-II: A revised measure of psychological inflexibility and experiential avoidance
DOI:10.1016/j.beth.2011.03.007
URL
PMID:22035996
[本文引用: 1]
The present research describes the development and psychometric evaluation of a second version of the Acceptance and Action Questionnaire (AAQ-II), which assesses the construct referred to as, variously, acceptance, experiential avoidance, and psychological inflexibility. Results from 2,816 participants across six samples indicate the satisfactory structure, reliability, and validity of this measure. For example, the mean alpha coefficient is .84 (.78–.88), and the 3- and 12-month test–retest reliability is .81 and .79, respectively. Results indicate that AAQ-II scores concurrently, longitudinally, and incrementally predict a range of outcomes, from mental health to work absence rates, that are consistent with its underlying theory. The AAQ-II also demonstrates appropriate discriminant validity. The AAQ-II appears to measure the same concept as the AAQ-I ( r = .97) but with better psychometric consistency.
Meta-analytic structural equation modeling: A two stage approach
DOI:10.1037/1082-989X.10.1.40
URL
PMID:15810868
[本文引用: 1]
To synthesize studies that use structural equation modeling (SEM), researchers usually use Pearson correlations (univariate r), Fisher z scores (univariate z), or generalized least squares (GLS) to combine the correlation matrices. The pooled correlation matrix is then analyzed by the use of SEM. Questionable inferences may occur for these ad hoc procedures. A 2-stage structural equation modeling (TSSEM) method is proposed to incorporate meta-analytic techniques and SEM into a unified framework. Simulation results reveal that the univariate-r, univariate-z, and TSSEM methods perform well in testing the homogeneity of correlation matrices and estimating the pooled correlation matrix. When fitting SEM, only TSSEM works well. The GLS method performed poorly in small to medium samples.
Fixed- and random-effects meta-analytic structural equation modeling: Examples and analyses in R
DOI:10.3758/s13428-013-0361-y
URL
PMID:23807765
[本文引用: 1]
Meta-analytic structural equation modeling (MASEM) combines the ideas of meta-analysis and structural equation modeling for the purpose of synthesizing correlation or covariance matrices and fitting structural equation models on the pooled correlation or covariance matrix. Cheung and Chan (Psychological Methods 10:40–64, 2005b , Structural Equation Modeling 16:28–53, 2009 ) proposed a two-stage structural equation modeling (TSSEM) approach to conducting MASEM that was based on a fixed-effects model by assuming that all studies have the same population correlation or covariance matrices. The main objective of this article is to extend the TSSEM approach to a random-effects model by the inclusion of study-specific random effects. Another objective is to demonstrate the procedures with two examples using the metaSEM package implemented in the R statistical environment. Issues related to and future directions for MASEM are discussed.
Meta-Analysis: A structural equation modeling approach
Acceptance and commitment therapy group for treatment-resistant participants: A randomized controlled trial
DOI:10.1016/j.jcbs.2014.04.005
URL
[本文引用: 3]
61Group-based ACT and CBT-based TAU for treatment-resistant clients were compared.61Both ACT and CBT-based TAU improved depression in clients post-intervention.61Only ACT maintained the improvements in depression at 6-month follow-up.61Both ACT and CBT-TAU reduced distress and improved quality of life at follow-up.61ACT theory consistent process was predictive of change at 6-month follow-up in ACT.
Acceptance and commitment therapy-based self-management versus psychoeducation training for staff caring for clients with a personality disorder: A randomized controlled trial
DOI:10.1521/pedi_2014_28_149
URL
PMID:24963830
[本文引用: 1]
Abstract People diagnosed with a personality disorder (PD) are often a stigmatized patient group. This can affect the care they receive, their progression, and the well-being of staff caring for them. Interventions targeted at health care professionals that aim to improve attitudes toward these patients and improve staff well-being do exist; however, evidence for their effectiveness is limited. The present study compared a self-management, Acceptance and Commitment Therapy-based training intervention (ACTr) with a Psychoeducation Training (PETr) intervention in their effectiveness in improving attitudes toward PD patients, staff-patient relations, and staff well-being. Both interventions were successful at improving attitudes and measures of staff-patient relations up to 6 months after training; however, staff well-being did not change for either group. The implications for staff training and future research are discussed.
Statistical power analysis for the behavioral sciences
.(2nd Edition.).
Considering meta-analysis, meaning, and metaphor: A systematic review and critical examination of “Third Wave” cognitive and behavioral therapies
DOI:10.1016/j.beth.2016.07.002
URL
PMID:27993339
[本文引用: 4]
61Scientific interest in “third wave” therapies has increased over time61Meta-analyses support the efficacy of the majority of therapies most commonly identified as “third wave”61Empirical studies are required to clarify the relationships among cognitive and behavioral therapies61The use of “third wave” as metaphor invites ongoing reflection and revision
Intervening variables in group-based acceptance & commitment therapy for severe health anxiety
DOI:10.1016/j.brat.2017.01.009 URL [本文引用: 2]
Reductions in experiential avoidance as a mediator of change in symptom outcome and quality of life in acceptance-based behavior therapy and applied relaxation for generalized anxiety disorder
DOI:10.1016/j.brat.2016.09.012
URL
PMID:27718414
[本文引用: 1]
61Examines changes in experiential avoidance across two behavioral treatments for GAD.61Greater change in EA significantly predicted change in worry across both treatments.61Greater change in EA significantly predicted quality of life across both treatments.61Results contribute to the literature on common mechanisms of change.
G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences
DOI:10.3758/BF03193146 URL [本文引用: 1]
Using session-by-session measurement to compare mechanisms of action for acceptance and commitment therapy and cognitive therapy
DOI:10.1016/j.beth.2011.07.004
URL
PMID:22440070
[本文引用: 3]
78 Patients (n=174) were randomly assigned to receive either ACT or CT. 78 A short assessment of theorized mediators and outcomes was administered before each session. 78 Utilization of change strategies relative to utilization of psychological acceptance strategies mediated outcome in CT. 78 Utilization of acceptance rather than change strategies mediated outcome in ACT. 78 Dysfunctional thinking, cognitive “defusion” and willingness to engage in difficult behaviors were equivalent mediators.
A randomized controlled effectiveness trial of acceptance and commitment therapy and cognitive therapy for anxiety and depression
DOI:10.1177/0145445507302202
URL
PMID:17932235
[本文引用: 3]
Abstract Acceptance and commitment therapy (ACT) has a small but growing database of support. One hundred and one heterogeneous outpatients reporting moderate to severe levels of anxiety or depression were randomly assigned to traditional cognitive therapy (CT) or to ACT. To maximize external validity, the authors utilized very minimal exclusion criteria. Participants receiving CT and ACT evidenced large, equivalent improvements in depression, anxiety, functioning difficulties, quality of life, life satisfaction, and clinician-rated functioning. Whereas improvements were equivalent across the two groups, the mechanisms of action appeared to differ. Changes in "observing" and "describing" one's experiences appeared to mediate outcomes for the CT group relative to the ACT group, whereas "experiential avoidance," "acting with awareness," and "acceptance" mediated outcomes for the ACT group. Overall, the results suggest that ACT is a viable and disseminable treatment, the effectiveness of which appears equivalent to that of CT, even as its mechanisms appear to be distinct.
The development and validation of the comprehensive assessment of acceptance and commitment therapy processes (CompACT)
DOI:10.1016/j.jcbs.2016.05.003
URL
[本文引用: 1]
61The CompACT’s items have better face and content validity than the AAQ-II’s items61The CompACT’s three factor structure reflects three dyadic ACT processes61The CompACT correlates with distress and wellbeing measures in predicted ways
How do mindfulness-based cognitive therapy and mindfulness-based stress reduction improve mental health and wellbeing? A systematic review and meta-analysis of mediation studies
DOI:10.1016/j.cpr.2015.01.006 URL [本文引用: 3]
A parallel group randomised open blinded evaluation of acceptance and commitment therapy for depression after psychosis: Pilot trial outcomes (ADAPT)
DOI:10.1016/j.schres.2016.11.026 URL [本文引用: 1]
Acceptance and commitment therapy-Do we know enough? Cumulative and sequential meta-analyses of randomized controlled trials
DOI:10.1016/j.jad.2015.10.053
URL
[本文引用: 2]
Highlights 61 ACT is an efficacious treatment for anxiety or depression. 61 Evidence is currently insufficient to conclude that ACT is more effective than CBT. 61 We report sample size estimates where sufficiency criteria have not been met. 61 Sequential Meta Analysis can increase confidence in quantitative review conclusions. Abstract Acceptance and Commitment Therapy (ACT) has accrued a substantial evidence base. Recent systematic and meta-analytic reviews suggest that ACT is effective compared to control conditions. However, these reviews appraise the efficacy of ACT across a broad range of presenting problems, rather than addressing specific common mental health difficulties. Focussing on depression and anxiety we performed a meta-analysis of trials of ACT. We incorporated sequential meta-analysis (SMA) techniques to critically appraise the sufficiency of the existing evidence base. Findings suggest that ACT demonstrates at least moderate group and pre-post effects for symptom reductions for both anxiety and depression. However using SMA findings are more qualified. There is currently insufficient evidence to confidently conclude that ACT for anxiety is efficacious when compared to active control conditions or as primary treatment for anxiety. Similarly, using SMA, there is currently insufficient evidence to suggest a moderate efficacy of ACT for depression compared to active control conditions. To stimulate further research we offer specific estimates of additional numbers of participants required to reach sufficiency to help inform future studies. We also discuss the appropriate strategies for future research into ACT for anxiety given the current evidence suggests no differential efficacy of ACT in the treatment of anxiety compared to active control conditions.
Long term follow up in children with anxiety disorders treated with acceptance and commitment therapy or cognitive behavioral therapy: Outcomes and predictors
Acceptance and commitment therapy versus cognitive behavior therapy for children with anxiety: Outcomes of a randomized controlled trial
DOI:10.1080/15374416.2015.1110822
URL
PMID:26998803
[本文引用: 2]
Abstract Acceptance and Commitment Therapy (ACT) has a growing empirical base in the treatment of anxiety among adults and children with other concerns. This study reports on the main outcomes of a randomized controlled trial of ACT and traditional cognitive behavioral therapy (CBT) in children with a Diagnostic and Statistical Manual of Mental Disorders (4th ed.) anxiety disorder. Participants were 193 children from urban Sydney, Australia, who were block-randomized to a 10-week group-based program of ACT or CBT or a 10-week waitlist control (WLC). Completers included 157 children (ACT = 54, CBT = 57, WLC = 46; M = 11 years, SD = 2.76; 78% Caucasian, 58% female). Pretreatment, posttreatment, and 3 months posttreatment assessments included clinician/self/parent-reported measures of anxiety, quality of life (QOL; anxiety interference, psychosocial and physical health-related QOL), and acceptance/defusion outcomes. Completer and intention-to-treat analyses revealed that ACT and CBT were both superior to WLC across outcomes, reflecting statistically and clinically significant differences, with gains maintained at 3 months posttreatment. Both completer and intention-to-treat analyses found ACT and CBT to produce similar outcomes. There was some support for ACT having greater effect sizes for QOL outcomes but not for avoidance/fusion. Although this study does not suggest that ACT is equivalent to CBT or should be adopted in its place, it does provide evidence that ACT might be another empirically supported treatment option for anxious youth. Further research is needed to replicate these findings.
Abstract 1. Beyond their existence in the behavior therapy tradition (broadly defined to encompass the entire range of behavioral and cognitive therapies, from clinical behavior analysis to cognitive therapy), no single factor unites the methods presented in this
Acceptance and commitment therapy: Model, processes and outcomes
DOI:10.1016/j.brat.2005.06.006
URL
PMID:16300724
[本文引用: 6]
The present article presents and reviews the model of psychopathology and treatment underlying Acceptance and Commitment Therapy (ACT). ACT is unusual in that it is linked to a comprehensive active basic research program on the nature of human language and cognition (Relational Frame Theory), echoing back to an earlier era of behavior therapy in which clinical treatments were consciously based on basic behavioral principles. The evidence from correlational, component, process of change, and outcome comparisons relevant to the model are broadly supportive, but the literature is not mature and many questions have not yet been examined. What evidence is available suggests that ACT works through different processes than active treatment comparisons, including traditional Cognitive-Behavior Therapy (CBT). There are not enough well-controlled studies to conclude that ACT is generally more effective than other active treatments across the range of problems examined, but so far the data are promising.
Open, aware, and active: Contextual approaches as an emerging trend in the behavioral and cognitive therapies
DOI:10.1146/annurev-clinpsy-032210-104449
URL
PMID:21219193
[本文引用: 2]
A wave of new developments has occurred in the behavioral and cognitive therapies that focuses on processes such as acceptance, mindfulness, attention, or values. In this review, we describe some of these developments and the data regarding them, focusing on information about components, moderators, mediators, and processes of change. These "third wave" methods all emphasize the context and function of psychological events more so than their validity, frequency, or form, and for these reasons we use the term "contextual cognitive behavioral therapy" to describe their characteristics. Both putative processes, and component and process evidence, indicate that they are focused on establishing a more open, aware, and active approach to living, and that their positive effects occur because of changes in these processes.
Experience sampling method: Measuring the quality of everyday life
Quantifying heterogeneity in a meta-analysis
DOI:10.1002/(ISSN)1097-0258 URL [本文引用: 2]
Acceptance and mindfulness-based therapy: New wave or old hat?
DOI:10.1016/j.cpr.2007.09.003
URL
PMID:17904260
[本文引用: 1]
Some contemporary theorists and clinicians champion acceptance and mindfulness-based interventions, such as Acceptance and Commitment Therapy (ACT), over cognitive ehavioral therapy (CBT) for the treatment of emotional disorders. The objective of this article is to juxtapose these two treatment approaches, synthesize, and clarify the differences between them. The two treatment modalities can be placed within a larger context of the emotion regulation literature. Accordingly, emotions can be regulated either by manipulating the evaluation of the external or internal emotion cues (antecedent-focused emotion regulation) or by manipulating the emotional responses (response-focused emotion regulation). CBT and ACT both encourage adaptive emotion regulation strategies but target different stages of the generative emotion process: CBT promotes adaptive antecedent-focused emotion regulation strategies, whereas acceptance strategies of ACT counteract maladaptive response-focused emotion regulation strategies, such as suppression. Although there are fundamental differences in the philosophical foundation, ACT techniques are fully compatible with CBT and may lead to improved interventions for some disorders. Areas of future treatment research are discussed.
The effectiveness of an acceptance and commitment therapy self-help intervention for chronic pain
DOI:10.1097/AJP.0b013e3181cf59ce
URL
PMID:20473046
[本文引用: 1]
Abstract OBJECTIVE: To evaluate the effectiveness of an Acceptance Commitment Therapy based self-help book for people with chronic pain. METHOD: This was a randomized 2 group study design. Over a 6-week period, 6 participants read the self-help book and completed exercises from it with weekly telephone support whereas 8 others formed a wait-list control group. Subsequently, 5 of the wait-list participants completed the intervention. Participants completed preintervention and postintervention questionnaires for acceptance, values illness, quality of life, satisfaction with life, depression, anxiety, and pain. Initial outcome data were collected for 8 control participants and 6 intervention participants. Including the wait-list controls, a total of 11 participants completed preintervention and postintervention measures. Whilst completing the self-help intervention, each week participants' rated the content of the book according to reading level and usefulness, and their comprehension of the content was also assessed. RESULTS: Compared with controls, participants who completed the book showed improved quality of life and decreased anxiety. When data from all the treatment participants were pooled, those who completed the intervention showed statistically significant improvements (with large effect sizes) for acceptance, quality of life, satisfaction with life, and values illness. Medium effect sizes were found for improvements in pain ratings. CONCLUSIONS: These findings support the hypothesis that using the self-help book, with minimal therapist contact adds value to the lives of people who experience chronic pain.
Acceptance and commitment therapy as a novel treatment for eating disorders: An initial test of efficacy and mediation
DOI:10.1177/0145445513478633 URL [本文引用: 1]
Mediators and mechanisms of change in psychotherapy research
DOI:10.1146/annurev.clinpsy.3.022806.091432 URL [本文引用: 3]
Processes of change in acceptance and commitment therapy and applied relaxation for long-standing pain
DOI:10.1002/ejp.754
URL
PMID:26684472
[本文引用: 3]
Background The utility of cognitive behavioural (CB) interventions for chronic pain has been supported in numerous studies. This includes Acceptance and Commitment Therapy (ACT), which has gained increased empirical support. Previous research suggests that improvements in pain catastrophizing and psychological inflexibility are related to improvements in treatment outcome in this type of treatment. Although a few studies have evaluated processes of change in CB-interventions, there is a particular need for mediation analyses that use multiple assessments to model change in mediators and outcome over time, and that incorporate the specified timeline between mediator and outcome in the data analytic model. Methods This study used session-to-session assessments to evaluate if psychological inflexibility, catastrophizing, and pain intensity mediated the effects of treatment on pain interference. Analyses were based on data from a previously conducted randomized controlled trial ( n = 60) evaluating the efficacy of ACT and Applied Relaxation (AR). A moderated mediation model based on linear mixed models was used to analyse the data. Results Neither catastrophizing nor pain intensity mediated changes in pain interference for any of the treatments. In contrast, psychological inflexibility mediated effects on outcome in ACT but not in AR. Conclusions Results add to previous findings illustrating the role of psychological inflexibility as a mediator in ACT.
Optimizing well-being: The empirical encounter of two traditions
DOI:10.1037/0022-3514.82.6.1007
URL
PMID:12051575
[本文引用: 1]
Abstract Subjective well-being (SWB) is evaluation of life in terms of satisfaction and balance between positive and negative affect; psychological well-being (PWB) entails perception of engagement with existential challenges of life. The authors hypothesized that these research streams are conceptually related but empirically distinct and that combinations of them relate differentially to sociodemographics and personality. Data are from a national sample of 3,032 Americans aged 25-74. Factor analyses confirmed the related-but-distinct status of SWB and PWB. The probability of optimal well-being (high SWB and PWB) increased as age, education, extraversion, and conscientiousness increased and as neuroticism decreased. Compared with adults with higher SWB than PWB. adults with higher PWB than SWB were younger, had more education, and showed more openness to experience.
Randomized controlled trial of acceptance and commitment therapy for distress and Impairment in OEF/OIF/OND veterans
DOI:10.1037/tra0000127 URL [本文引用: 1]
Web-based acceptance and commitment therapy for depressive symptoms with minimal support: A randomized controlled trial
DOI:10.1177/0145445515598142 URL [本文引用: 3]
Using brief cognitive restructuring and cognitive defusion techniques to cope with negative thoughts
DOI:10.1177/0145445515621488
URL
PMID:26685210
[本文引用: 1]
ABSTRACT Negative thoughts, experienced by 80% to 99% of the non-clinical population, have been linked to the development of psychopathology. The current study aimed to compare a cognitive restructuring and cognitive defusion technique for coping with a personally relevant negative thought. Over a 5-day period, participants used either a restructuring, defusion, or control strategy to manage a negative thought. Pre- and post-intervention participants reported (a) believability of the thought, (b) discomfort associated with the thought, (c) negativity associated with the thought, and (d) willingness to experience the thought. Daily online questionnaires assessing the total frequency of negative thought intrusions and their level of willingness to experience the negative thought were also used. Also, 10 positive and negative self-statements were rated on the same scales, and self-report measures of mood and psychological flexibility were completed. Findings indicated that defusion lowered believability, increased comfort and willingness to have the target thought, and increased positive affect significantly more than the control and cognitive restructuring. Within groups, cognitive restructuring also made significant gains in target thought discomfort, negativity, and "willingness to have" in the same direction as defusion but the no-instruction control did not. Negative thought frequency was reduced in the defusion group, maintained in the restructuring group, and increased in the no-instruction control group. Similar trends emerged from the secondary outcome measures, that is, the effects of the strategies on the positive and negative self-statements. The current findings support the efficacy of using defusion as a strategy for managing negative thoughts.
Mechanisms of change in psychotherapy for depression: An empirical update and evaluation of research aimed at identifying psychological mediators
DOI:10.1016/j.cpr.2016.09.004
URL
PMID:27770716
[本文引用: 4]
61Little is known about the psychological mechanisms of psychotherapy for depression.61Themechanism questionhas motivated dozens of investigations of mediation.61We provide an empirical update and critical evaluation of this body of research.61Research is heterogeneous and unsatisfactory in methodological respect.61Psychotherapy might be too complex to be explained in simple models of change.
Evaluating an adjunctive mobile app to enhance psychological flexibility in acceptance and commitment therapy
DOI:10.1177/0145445517719661
URL
PMID:28689449
[本文引用: 2]
The primary aims of this study were to evaluate the feasibility and potential efficacy of a novel adjunctive mobile app designed to enhance the acquisition, strengthening, and generalization of acceptance and commitment therapy (ACT) skills being taught in therapy. A sample of 14 depressed/anxious clients receiving ACT used the ACT Daily app for two weeks in a pre-post, open trial design. Participants reported a high degree of program satisfaction. Clients significantly improved over the two-week period on depression and anxiety symptoms as well as a range of psychological inflexibility measures. Analyses of mobile app data indicated effects of ACT Daily skill coaching on in-the-moment measures of inflexibility and symptoms, with unique effects found for acceptance and mindfulness. Adjunctive ACT mobile apps appear promising in enhancing therapy effects on psychological inflexibility and outcomes. A tailored skill coaching approach like ACT Daily based on randomly prompted assessments may be especially promising.
Web-based acceptance and commitment therapy for mental health problems in college students: A randomized controlled trial
DOI:10.1177/0145445516659645 URL [本文引用: 3]
Web-based self-help for preventing mental health problems in universities: Comparing acceptance and commitment training to mental health education
DOI:10.1002/jclp.22254
URL
PMID:26784010
[本文引用: 3]
Abstract OBJECTIVE: This study sought to test the feasibility of a web-based Acceptance and Commitment Training (ACT) prototype prevention program called ACT on College Life (ACT-CL). METHOD: A sample of 234 university students was randomized to either the ACT-CL website or a mental health education (MHE) website. RESULTS: Findings indicated a lower level of user engagement and satisfaction ratings with the prototype of ACT-CL than the MHE website. There were no significant differences between conditions on outcome measures at post or follow-up. However, statistical trends suggested the MHE condition actually led to greater remission of severe symptoms than the ACT-CL condition among those with severe symptoms at baseline. There were no differences between conditions on ACT process of change measures. Changes in psychological flexibility were predictive of changes in mental health across conditions, but relations dissipated over time. Furthermore, greater engagement in some components of ACT-CL predicted improvements in psychological flexibility, though not on mental health outcomes. CONCLUSIONS: The effects of the ACT-CL program on mental health outcomes and ACT process measures were largely equivalent to those of an education website, although there was a lower level of program engagement with ACT-CL. Findings are discussed in the context of feasibility issues and lessons learned for program revisions. 2016 Wiley Periodicals, Inc.
Feasibility of a prototype web-based acceptance and commitment therapy prevention program for college students
DOI:10.1080/07448481.2013.843533
URL
PMID:24313693
[本文引用: 1]
Objective: This study examined the feasibility of a prototype Web-based acceptance and commitment therapy (ACT) program for preventing mental health problems among college students. Participants: Undergraduate first-year students (N = 76) participated between May and November 2011. Methods: Participants were randomized to ACT or a waitlist, with assessments conducted at baseline, posttherapy, and 3-week follow-up. Waitlist participants accessed the program after the second assessment. Results: Program usability/usage data indicated high program acceptability. Significant improvements were found for ACT knowledge, education values, and depression with ACT relative to waitlist. Subgroup analyses indicated that ACT decreased depression and anxiety relative to waitlist among students with at least minimal distress. Within the ACT condition, significant improvements were observed from baseline to 3-week follow-up on all outcome and process measures. Conclusions: Results provide preliminary support for the feasibility of a Web-based ACT prevention program.
Practical meta-analysis. Applied social research methods series
The value of psychological flexibility: Examining psychological mechanisms underpinning a cognitive behavioural therapy intervention for burnout
DOI:10.1080/02678373.2013.782157
URL
[本文引用: 1]
Little is known of the mechanisms by which interventions for burnout work. Employees of a UK government department were randomly assigned to either a worksite group-based CBT intervention called Acceptance and Commitment Therapy (ACT; n=43), which aimed to increase participants' psychological flexibility, or a waiting list control group (n=57). The ACT group received three half-day sessions of training spread over two and a half months. Data were collected at baseline (T1), at the beginning of the second (T2) and third (T3) workshops, and at six months' follow up (T4). Consistent with ACT theory, analyses revealed that, in comparison to the control group, a significant increase in psychological flexibility from T2 to T3 in the ACT group mediated the subsequent T2 to T4 decrease in emotional exhaustion in that group. Consistent with a theory of emotional burnout development, this significant decrease in emotional exhaustion from T2 to T4 in the ACT group appeared to prevent the significant T3 to T4 increase in depersonalization seen in the control group. Strain also decreased from T2 to T3 in the ACT group only, but no mediator of that improvement was identified. Implications for theory and practice in the fields of ACT and emotional burnout are discussed.
The differential effects of weekly, monthly, and bimonthly administrations of the beck depression inventory-II: Psychometric properties and clinical implications
DOI:10.1016/S0005-7894(05)80075-9
URL
[本文引用: 1]
Research suggests that scores decrease over time when valid self-report depression instruments are administered repeatedly without intervention to nonclinical participants. Existing research has not addressed whether similar decreases occur with differential retest intervals and whether this decrease represents error or a “true” decrease in symptomatology. In the current study, nonclinical participants were randomly assigned to complete the Beck Depression Inventory-II at weekly, monthly, or bimonthly intervals. Scores were found to significantly decrease for the weekly administration group only. Lower scores were found to be the result of a measurement effect and the frequency of administration. Limitations as well as research and clinical implications are discussed.
Effectiveness of group acceptance and commitment therapy for fibromyalgia: A 6-month randomized controlled trial (EFFIGACT study)
DOI:10.1016/j.pain.2013.12.029
URL
PMID:24378880
[本文引用: 4]
In the last decade, there has been burgeoning interest in the effectiveness of third-generation psychological therapies for managing fibromyalgia (FM) symptoms. The present study examined the effectiveness of acceptance and commitment therapy (ACT) on functional status as well as the role of pain acceptance as a mediator of treatment outcomes in FM patients. A total of 156 patients with FM were enrolled at primary health care centers in Zaragoza, Spain. The patients were randomly assigned to a group-based form of ACT (GACT), recommended pharmacological treatment (RPT; pregabalin + duloxetine), or wait list (WL). The primary end point was functional status (measured with the Fibromyalgia Impact Questionnaire, FIQ). Secondary end points included pain catastrophizing, pain acceptance, pain, anxiety, depression, and health-related quality of life. The differences between groups were calculated by linear mixed-effects (intention-to-treat approach) and mediational models through path analyses. Overall, GACT was statistically superior to both RPT and WL immediately after treatment, and improvements were maintained at 6months with medium effect sizes in most cases. Immediately after treatment, the number needed to treat for 20% improvement compared to RPT was 2 (95% confidence interval 1.2 2.0), for 50% improvement 46, and for achieving a status of no worse than mild impaired function (FIQ total score <39) also 46. Unexpectedly, 4 of the 5 tested path analyses did not show a mediation effect. Changes in pain acceptance only mediated the relationship between study condition and health-related quality of life. These findings are discussed in relation to previous psychological research on FM treatment.
Mediation analysis
DOI:10.1146/annurev.psych.58.110405.085542 URL [本文引用: 3]
Interpersonal problems, mindfulness, and therapy outcome in an acceptance-based behavior therapy for generalized anxiety disorder
DOI:10.1080/16506073.2015.1060255
URL
PMID:26228536
[本文引用: 1]
Objective:To better understand the role interpersonal problems play in response to two treatments for generalized anxiety disorder (GAD); an acceptance-based behavior therapy (ABBT) and applied relaxation (AR), and to examine how the development of mindfulness may be related to change in interpersonal problems over treatment and at follow-up.Method:Eighty-one individuals diagnosed with GAD (65.4% female, 80.2% identified as white, average age 32.92) were randomized to receive 16 sessions of either ABBT or AR. GAD severity, interpersonal problems, and mindfulness were measured at pre-treatment, post-treatment, 6-month follow-up, and 12-month follow-up.Results:Mixed effect regression models did not reveal any significant effects of pre-treatment interpersonal problems on GAD severity over treatment. After controlling for post-treatment GAD severity, remaining post-treatment interpersonal problems predicted 6- but not 12-month GAD severity. Participants in both conditions experienced a large decrease in interpersonal problems over treatment. Increases in mindfulness over treatment and through follow-up were associated with decreases in interpersonal problems, even when accounting for reductions in overall GAD severity.Conclusions:Interpersonal problems may be an important target of treatment in GAD, even if pre-treatment interpersonal problems are not predictive of outcome. Developing mindfulness in individuals with GAD may help ameliorate interpersonal difficulties among this population.
Factors affecting adoption of online banking: A meta-analytic structural equation modeling study
DOI:10.1016/j.im.2014.11.002
URL
[本文引用: 3]
Despite the potential benefits that online banking offers consumers, it has low adoption rate. We systematically review online banking adoption literature to propose two research models of factors affecting pre-adoption and post-adoption of the online banking. To test our proposed models, we applied a two-stage random-effects meta-analytic structural equation modeling method to data collected from 25,265 cases from primary empirical studies of online banking adoption. Our findings show that ten factors affect consumers’ adoption of the online banking. Furthermore, we show that the relative importance of these factors differs depending on consumers’ pre-adoption and post-adoption of the online banking.
Estimating effect sizes from pretest-posttest-control group designs
DOI:10.1177/1094428106291059
URL
[本文引用: 1]
Previous research has recommended several measures of effect size for studies with repeated measurements in both treatment and control groups. Three alternate effect size estimates were compared in terms of bias, precision, and robustness to heterogeneity of variance. The results favored an effect size based on the mean pre-post change in the treatment group minus the mean pre-post change in the control group, divided by the pooled pretest standard deviation.
Efficacy of the third wave of behavioral therapies: A systematic review and meta-analysis
DOI:10.1016/j.brat.2007.12.005
URL
PMID:18258216
[本文引用: 1]
During the last two decades a number of therapies, under the name of the third wave of cognitive behavior therapy (CBT), have been developed: acceptance and commitment therapy (ACT), dialectical behavior therapy (DBT), cognitive behavioral analysis system of psychotherapy (CBASP), functional analytic psychotherapy (FAP), and integrative behavioral couple therapy (IBCT). The purposes of this review article of third wave treatment RCTs were: (1) to describe and review them methodologically, (2) to meta-analytically assess their efficacy, and (3) to evaluate if they currently fulfil the criteria for empirically supported treatments. There are 13 RCTs both in ACT and DBT, 1 in CBASP, 2 in IBCT, and none in FAP. The conclusions that can be drawn are that the third wave treatment RCTs used a research methodology that was significantly less stringent than CBT studies; that the mean effect size was moderate for both ACT and DBT, and that none of the third wave therapies fulfilled the criteria for empirically supported treatments. The article ends with suggestions on how to improve future RCTs to increase the possibility of them becoming empirically supported treatments.
The efficacy of acceptance and commitment therapy: An updated systematic review and meta-analysis
DOI:10.1016/j.brat.2014.07.018
URL
PMID:25193001
[本文引用: 3]
61ACT RCTs had a number of important methodological problems.61The overall effect size was small.61The ES for ACT-CBT comparisons was not significant.61ACT did not fulfill criteria for well-established treatment for any disorder.
Evaluating coding decisions
In H. Cooper., & L. V. Hedges (Eds.), The handbook of research synthesis(pp. 139-162).
Acceptance and commitment therapy: A meta-analytic review
DOI:10.1159/000190790 URL [本文引用: 1]
Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models
DOI:10.3758/BRM.40.3.879 URL [本文引用: 2]
Effectiveness and mechanism of internet-based self-help intervention for depression: The Chinese version of MoodGYM
抑郁症网络化自助干预的效果及作用机制——以汉化MoodGYM为例
DOI:10.3724/SP.J.1041.2016.00818
URL
[本文引用: 2]
抑郁症是全球性的重要公共健康问题,抑郁症的网络化认知行为治疗近年来备受关注。本研究采用随机对照组试验考察抑郁症网络化干预程序Mood GYM中文版对中国大学生抑郁患者的在线干预效果,并且使用多重中介模型同时探索了基于临床实践提出的认知歪曲(ATQ和DAS)与认知领域研究发现的解释偏差(SST)在抑郁症网络化认知行为治疗中的作用机制。结果发现:(1)相较之对照组,Mood GYM对中国大学生抑郁的网络化自助干预具有中到大的效果量(CES-D,d=0.93;PHQ-9,d=0.79);(2)Mood GYM也显著降低抑郁患者的负性自动思维(ATQ)、消极解释偏差(SST)和功能失调性态度(DAS);(3)自动思维(ATQ)和消极解释偏差(SST)二者的改变在抑郁症网络化认知行为治疗效果中起中介作用,功能失调性态度改变的中介效应不显著。抑郁症的网络化干预还存在着诸如脱落率较高等多种局限,推荐作为传统心理治疗的额外补充手段,也可作为梯度治疗模型的自助式初级干预。
Improving psychological adjustment among late-stage ovarian cancer patient: Examining the role of avoidance in treatment
DOI:10.1016/j.cbpra.2012.01.003
URL
[本文引用: 3]
78 We examined the efficacy of ACT in treating distress among patients with advanced cancer. 78 ACT was at least as effective as TAU on all measures of psychological distress. 78 Avoidance plays a significant mediating role in treatment outcomes.
Publication bias in meta-analysis: Prevention, assessment and adjustments
Acceptance and commitment therapy versus traditional cognitive behavioral therapy: A systematic review and meta-analysis of current empirical evidence
DOI:10.1007/BF02266700
URL
[本文引用: 1]
Cognitive behavioral therapy (CBT) is widely considered as the approach to psychotherapy with...
Methods of meta-analysis: Correcting error and bias in research findings (3rd ed.)
The effectiveness of an act informed intervention for managing stress and improving therapist qualities in clinical psychology trainees
DOI:10.1002/jclp.2012.68.issue-6 URL [本文引用: 3]
Mechanisms of change: Exploratory outcomes from a randomised controlled trial of acceptance and commitment therapy for anxious adolescents
DOI:10.1016/j.jcbs.2014.09.001 URL [本文引用: 3]
Acceptance rationale and increasing pain tolerance: Acceptance-based and Fear-based practice
Internet-based guided self-help intervention for chronic pain based on acceptance and commitment therapy: A randomized controlled trial
DOI:10.1007/s10865-014-9579-0 URL [本文引用: 1]
Acceptance and commitment therapy modules: Differential impact on treatment processes and outcomes
DOI:10.1016/j.brat.2015.12.001 URL [本文引用: 2]
Theory testing: Combining psychometric meta‐analysis and structural equations modeling
DOI:10.1111/peps.1995.48.issue-4 URL [本文引用: 1]
The great psychotherapy debate: Models, methods, and findings
The great psychotherapy debate: The evidence for what makes psychotherapy work (2nd ed.)
Acceptance and commitment therapy (ACT) for clinically distressed health care workers: Waitlist-controlled evaluation of an ACT workshop in a routine practice setting
DOI:10.1111/bjc.2018.57.issue-1 URL [本文引用: 1]
Acceptance and commitment therapy versus tinnitus retraining therapy in the treatment of tinnitus: A randomised controlled trial
DOI:10.1016/j.brat.2011.08.001 URL [本文引用: 1]
A randomized, controlled trial of acceptance and commitment therapy and cognitive-behavioral therapy for chronic pain
DOI:10.1016/j.pain.2011.05.016 URL [本文引用: 1]
A feasibility study of acceptance and commitment therapy for emotional dysfunction following psychosis
DOI:10.1016/j.brat.2011.09.003 URL [本文引用: 1]
Can exposure and acceptance strategies improve functioning and life satisfaction in people with chronic pain and whiplash-associated disorders (WAD)? A randomized controlled trial
DOI:10.1080/16506070802078970 URL [本文引用: 1]
Acceptance and commitment therapy for fibromyalgia: A randomized controlled trial
DOI:10.1002/ejp.2013.17.issue-4 URL [本文引用: 2]
Using acceptance and commitment therapy to increase self-compassion: A randomized controlled trial
DOI:10.1016/j.jcbs.2014.09.002 URL [本文引用: 2]
A randomized controlled trial of acceptance and commitment therapy for aggressive behavior
DOI:10.1037/a0037946 URL [本文引用: 1]
The theoretical background, empirical study and future development of the acceptance and commitment therapy
接纳与承诺疗法的理论背景、实证研究与未来发展
Processes of change in acceptance and commitment therapy and cognitive therapy for depression: A mediation reanalysis of Zettle and Rains
DOI:10.1177/0145445511398344 URL [本文引用: 2]

{kind=link}
{kind=link}
{kind=link}
{kind=link}